It must be about six years since I wrote about Parkinson’s Disease [PD]and chronic kidney disease. It’s a biggie for me because both my brothers had this disease. One is now deceased. The other presently suffers Parkinson’s dementia. Hmm, three siblings: two with PD, one with CKD. Time to see what the connection, if any, is.
“Reduced kidney function in patients with type 2 diabetes (T2D) may increase the risk of developing Parkinson disease (PD), according to study findings published in Parkinsonism & Related Disorders.
Affecting 1 in 11 adults worlwide [stet], T2D shares several pathophysiology [Gail here. That means disease or injury related disorder of the physiological processes.] similarities with PD, including mitochondrial dysfunction, endoplasmic reticulum stress, inflammation, and altered metabolism.”
If you’re anything like me, you need more of these terms defined. The Children’s Hospital of Philadelphia offers the definition of mitochondrial disorder:
“Mitochondrial disease, or mitochondrial disorder, refers to a group of disorders that affect the mitochondria, which are tiny compartments that are present in almost every cell of the body. The mitochondria’s main function is to produce energy. More mitochondria are needed to make more energy, particularly in high-energy demand organs such as the heart, muscles, and brain. When the number or function of mitochondria in the cell are disrupted, less energy is produced and organ dysfunction results.”
Once again, it’s clear that I’m not a doctor [and never have claimed to be one]. I am learning along with you. While I’d seen the term ’mitochondrial disorder’ before and thought I knew what It meant, I didn’t.
“ER stress occurs when the capacity of the ER to fold proteins becomes saturated.”
As for altered metabolism, we know what altered means so let’s define metabolism. Thank you to my favorite dictionary, the Merriam-Webster:
“the sum of the processes in the buildup and destruction of protoplasm
specifically:the chemical changes in living cells by which energy is provided for vital processes and activities and new material is assimilated”
I have type 2 diabetes, so this study does mean something to me. It might mean something to you if you also have type 2 diabetes and CKD. I’m going to mention the study to my nephrologist when next I see him.
“However, neurological consequences are also attributed to this disease. Among these, recent large epidemiological studies have demonstrated an increased risk for Parkinson’s disease (PD) in patients with CKD.”
Oh no, maybe I’ll come to PD from a different point of origin than those of my brothers. Come to think of it, I don’t know how they developed PD. Anyway, I don’t want to come to PD from any point of origin.
I wanted to know more, as usual. While not exactly what I’d been looking for the University of Florida Health made an interesting comparison between PD and CKD:
“This situation of a ‘threshold’ of cell loss that must be eclipsed for appearance of symptoms can be compared to what may occur in patients who experience kidney failure. When a kidney begins to malfunction, approximately 75% or more of its cells are lost, and those cells are unrecoverable. Frustratingly, for kidney failure failure [stet] patients, the routine laboratory tests are almost never abnormal, and only hint abnormality when the failure process has already begun. In Parkinson’s disease, as in kidney failure, a ‘threshold’ of cells must be lost before one manifests symptoms.”
Never have I ever been so loathe at a possible comparison between my big brothers and me. It hit too close to home and, somehow, made me miss my brothers even more.
“… we explored the association of CKD and PD and linked the components of the former to propose potential pathways explaining a future increased risk for PD, where renin-angiotensin system, oxidative stress, and inflammation have a main role.”
Wait a minute. Renin-angiotensin system? That sounds familiar. Britannica reminds us what it is:
“renin-angiotensin system, physiological system that regulates blood pressure.
Renin is an enzymesecreted into the blood from specialized cells that encircle the arterioles at the entrance to the glomeruli of the kidneys (the renal capillary networks that are the filtration units of the kidney). The renin-secreting cells, which compose the juxtaglomerular apparatus, are sensitive to changes in blood flow and blood pressure. The primary stimulus for increased renin secretion is decreased blood flow to the kidneys, which may be caused by loss of sodium and water (as a result of diarrhea, persistent vomiting, or excessive perspiration) or by narrowing of a renal artery.”
And this system has a main role in possible increased risk for PD???? This is getting too close for comfort. However, the same article concluded:
“More preclinical studies are needed to confirm the potential link of CKD conditions and future PD risk, whereas more interventional studies targeting this association are warranted to confirm their potential benefit in PD.”
I was glad to read that. Personally, I’m not willing to take on Parkinson’s in addition to my CKD and type 2 diabetes. Then again, is anyone? I hope I’ve both opened a new topic for you and put your mind at ease.
A very active reader – who happens to be a transplantee – asked me to write about spilling protein. As a CKD patient, I’ve never been told I was doing that. However, one of my daughters was told she was spilling urine. She does not have chronic kidney disease. Hmmm.
Way back in 2020, I became interested in proteinuria simply because, while I knew the meaning of the word, I didn’t really know what the definition meant. In other words, I could break down the parts of the word [protein and urine] but didn’t get what they meant when combined. I found this information from The Mayo Clinic useful in helping me to understand:
“Protein in urine — known as proteinuria (pro-tee-NU-ree-uh) — is excess protein found in a urine sample. Protein is one of the substances identified during a test to analyze the content of your urine (urinalysis).
Low levels of protein in urine are normal. Temporarily high levels of protein in urine aren’t unusual either, particularly in younger people after exercise or during an illness.
Persistently high levels of protein in urine may be a sign of kidney disease.”
Oh, maybe this explained why my daughter was spilling protein into her urine. Perhaps she was ill or had just exercised before the test not realizing that would affect the results.
I wondered precisely what it was that healthy kidneys did do. The American Kidney Fund explained a bit more:
“Healthy kidneys remove extra fluid and waste from your blood, but let proteins and other important nutrients pass through and return to your blood stream. When your kidneys are not working as well as they should, they can let some protein (albumin) escape through their filters, into your urine. When you have protein in your urine, it is called proteinuria …. Having protein in your urine can be a sign of nephrotic syndrome, or an early sign of kidney disease.”
There’s another reason you don’t want to have proteinuria as WebMD clarifies:
“Protein is an important component of every cell in the body. Hair and nails are mostly made of protein. Your body uses protein to build and repair tissues. You also use protein to make enzymes, hormones, and other body chemicals. Protein is an important building block of bones, muscles, cartilage, skin, and blood.”
I thought I’d throw this tidbit in since I just spent two weeks writing about biopsies. The paper Patient education: Kidney (renal) biopsy (Beyond the Basics) written by William L Whittier, MD, FASN and Stephen M Korbet, MD, MACP published on UpToDate informs us:
““The following are the most common reasons for kidney biopsy. You may have one or more of these problems, but not everyone with these problems needs a kidney biopsy:
●Blood in the urine (called hematuria). …
●Protein in the urine (called proteinuria) – This occurs in many people with kidney problems. A kidney biopsy may be recommended if you have high or increasing levels of protein in the urine or if you have proteinuria along with other signs of kidney disease….
●Problems with kidney function – If your kidneys suddenly or slowly stop functioning normally, a kidney biopsy may be recommended, especially if the cause of your kidney problem is unclear.”
Take a look at the second reason for having a biopsy.
I think it would make sense to learn how the kidney becomes so damaged that it allows protein, which is meant to return to the blood, to spill into the urine. I turned to the Cleveland Clinic to find out:
“Protein gets into the urine if the kidneys aren’t working properly. Normally, glomeruli, which are tiny loops of capillaries (blood vessels) in the kidneys, filter waste products and excess water from the blood.
Glomeruli pass these substances, but not larger proteins and blood cells, into the urine. If smaller proteins sneak through the glomeruli, tubules (long, thin, hollow tubes in the kidneys) recapture those proteins and keep them in the body.
However, if the glomeruli or tubules are damaged, if there is a problem with the reabsorption process of the proteins, or if there is an excessive protein load, the proteins will flow into the urine.”
‘Excessive protein load’ That’s why our protein intake is limited. We do not want to overwork and possibly damage our kidneys by relying on a diet of burgers, chicken, steak, and salmon. This doesn’t mean you cannot have these or similar foods; simply that you need to limit them each day. Your nephrologist or renal dietitian will tell you how much protein per day is the right amount for you.
I wondered if that was the only cause of damaged kidneys. According to the Mayo Clinic, it’s not. There’s also:
“Type 1 or type 2 diabetes
High blood pressure
Glomerulonephritis (gloe-mer-u-low-nuh-FRY-tis), an inflammation of the kidney’s filtering units (glomeruli)
Interstitial nephritis (in-tur-STISH-ul nuh-FRY-tis), an inflammation of the kidney’s tubules and surrounding structures
Polycystic kidney disease or other inherited kidney diseases
Prolonged obstruction of the urinary tract, from conditions such as enlarged prostate, kidney stones and some cancers
Vesicoureteral (ves-ih-koe-yoo-REE-tur-ul) reflux, a condition that causes urine to back up into your kidneys
Recurrent kidney infection, also called pyelonephritis (pie-uh-low-nuh-FRY-tis)”
Remember, CKD is at least three months of your kidney function declining.
Since the question was asked by a transplantee, let’s see if there’s anything to add specifically for this group of people. New York based Nao Medical made it easy to understand:
“There are several factors that can contribute to the development of proteinuria in kidney transplant patients. These include:
Rejection of the transplanted kidney
Infection
Medications
High blood pressure
Diabetes”
Transplantees: Take note that rejection is not the only cause of proteinuria.
As for the treatment of proteinuria in transplantees, I am confused. I found research that stated Vitamin D would do the trick, others that recommended statins, and still other that said antihypertension drugs would help. I remind you that I am not a doctor and have never claimed to be one. In other words, speak with your nephrologist to discover which treatment is the best for your proteinuria.
I learned quite a bit today and hope you did, too.
Now that I have your attention, I wonder if you’ve ever heard of the vagus nerve and its connection to your kidneys. It kept popping up in my dreams, so I thought it might be worth exploring. Of course, I needed to bring you along in my exploration.
Instead of going directly to my favorite dictionary, I turned to WebMD since I felt this term needed a simpler definition than even the dictionary could provide.
“The vagus (vagal) nerve is also known as the 10th cranial nerve or cranial nerve X. It starts in your medulla oblongata, a part of the brain that connects to the spinal cord, and splits off into many branches that extend down through your neck to your vital abdominal organs.
This long nerve makes up 3/4 of the nerve tissue in your parasympathetic nervous system. In fact, the vagus nerve is the longest of any of the 12 cranial nerves.”
Nice. But what does it actually do? I searched and found this explanation on Physiopedia, a UK charity organization that offers rehabilitation education:
“The vagus nerve has a very extensive distribution.
Sensory: Innervates the skin of the external acoustic meatus and the internal surfaces of the laryngopharynx and larynx. Provides visceral sensation to the heart and abdominal viscera.
Special Sensory: Provides taste sensation to the epiglottis and root of the tongue.
Motor: Provides motor innervation to the majority of the muscles of the pharynx, soft palate and larynx.
Parasympathetic: Innervates the smooth muscle of the trachea, bronchi and gastro-intestinal tract and regulates heart rhythm. Its cardiac branches act to slow the rate of heartbeat; its bronchial branch acts to constrict the bronchi; and its esophageal branches control involuntary muscles in the esophagus, stomach, gallbladder, pancreas, and small intestine, stimulating peristalsis and gastrointestinal secretions. …”
Wait a minute. What about the kidneys? InKidney helped out here. InKidney was formed by healthcare professionals that are concerned about the wide spread of kidney disease worldwide.
“Emotional stress can be associated with faster progression of CKD. The kidneys have both sympathetic and parasympathetic innervation. Acute stress can worsen kidney function, while relaxation practices can promote kidney health. Stimulating the vagus nerve can turn on the parasympathetic nervous system, improving renal blood flow and modulating inflammation in CKD. Stress reduction and the natural stimulation of the vagus nerve can help delay the progression of kidney disease.”
How about a reminder of what sympathetic and parasympathetic systems are. Thanks to The Cleveland Clinic for this information:
“Your sympathetic nervous system is part of your autonomic nervous system. It could be called your ‘automatic’ nervous system, as it is responsible for many functions that you don’t have to think about to control. This can include control of your heart rate, blood pressure, digestion, urination and sweating, among other functions.
Your sympathetic nervous system is best known for its role in responding to dangerous or stressful situations. In these situations, your sympathetic nervous system activates to speed up your heart rate, deliver more blood to areas of your body that need more oxygen or other responses to help your [sic] get out of danger.”
“Your parasympathetic nervous system is part of your autonomic nervous system. It could be called your ‘automatic’ nervous system, as it’s responsible for many functions that you don’t have to think about to control. This can include control of your heart rate, blood pressure, digestion, urination and sweating, among other functions.
The parasympathetic part of your autonomic nervous system balances your sympathetic nervous system. While your sympathetic nervous system controls your body’s ‘fight or flight’ response, your parasympathetic nervous system helps to control your body’s response during times of rest.”
Hopefully, these two definitions helped you to understand the connection between your kidneys and the vagus nerve. I must admit, they did help me.
Healthline gave me some insight into the varied possible symptoms of a damaged vagus nerve:
“Damage to the vagus nerve can result in a range of symptoms because the nerve is so long and affects many areas.
depression and anxiety in people with breathing problems or heart disease
The symptoms someone might have depend on what part of the nerve is damaged.”
I wanted to know how you stimulate the vagus nerve. I had a vision of a doctor reaching into a body incision and using their hands to do so. I doubt that’s how it’s done, though. Back to the ever helpful Cleveland Clinic for us:
“Meditation
Turn to this practice to help calm your mind and focus on deep breathing. While doing meditation, try extending your exhales, making them longer than your inhales. This will help slow your heart rate.
‘Meditation can regulate your autonomic nervous system,” says Dr. Estemalik. “It has a good effect on lowering rapid breathing, rapid heart rate and cortisol levels.’
Yoga can also be helpful for the same reasons. Just make sure you pay attention on your breathing.
Exercise
…. Working out and getting your body moving can affect your vagus nerve, research shows. Interval training and endurance training can increase your vagus nerve activity and improve your heart rate variability.
Massage
Research shows that reflexology (a kind of massage) can increase vagal tone and even decrease blood pressure.
‘Massage can reduce some of the heightened activity in the vagus nerve,’ says Dr. Estemalik.
Try giving yourself a foot massage by rotating your ankle, rubbing your sole in short strokes and gently stretching your toes back and forth.
Music
Music can help motivate us, bring us joy and tap into our emotions. When it comes to the vagus nerve, the research is mixed on how music affects it.
Your vagus nerve is connected to your vocal cords, the muscles at the back of your throat and passes through your inner ear.
Try humming or singing or just listening to calm, soothing music. Those sounds and vibrations may stimulate your vagus nerve.
Cold-water immersion
…. Research shows that cold-water immersion may help with stress by slowing your heart rate and directing blood flow to your brain. Try placing an ice pack on your face or neck or taking a cold shower.”
There is also a device that can be implanted under your skin, but I believe that is used for stroke victims, epilepsy, and migraines. That’s much more involved with this device, but that’s a whole other blog.
Remember: Stress leads to inflammation. Inflammation may lead to kidney disease.
I have a new painful condition but making the connection between chronic kidney disease and this condition had me laughing while seated at my computer. You’ll see. It is a warped connection. Ah, I haven’t told you what that condition is yet. It’s spinal stenosis.
Hold on there. Of course, I’ll explain what it is. Spinal simply means of or about the spine. Stenosis means narrowing. I’ll bet you’re glad I had a thorough English language education at Hunter College a long, long time ago.
We both know narrowing of the spine really doesn’t make sense, so let’s find a more precise definition of this condition. Hello, WebMD:
“Spinal stenosis is a condition, mostly in adults 50 and older, in which your spinal canal starts to narrow. This can cause pain and other problems.
Your spine is made up of a series of connected bones (or vertebrae) and shock-absorbing discs. It protects your spinal cord, a key part of the central nervous system that connects your brain to your body. The cord rests in the canal formed by your vertebrae.”
Not only does it occur in adults over 50, but it occurs more often in women. That’s me… well over 50 and a woman. I wondered why it occurs more often in women, but that’s a blog for another day.
Simply adding the word ‘canal’ made the definition clearer. So, what’s happening here is that the canal, not the spine itself, is narrowing. How? NYU‘s Langone Health, part of NYU – a #1 hospital – explains:
“For most people diagnosed with spinal stenosis, the spinal canal narrows because of degeneration in the spine that occurs as a natural part of aging. These degenerative changes most frequently affect the vertebral joints, also called facet joints, and the spongy discs that lie between vertebrae.
As the spine ages, intervertebral discs slowly lose fluid in a process called degenerative disc disease. Degeneration may cause a disc to bulge into the spinal canal, putting pressure on nerves or the spinal cord. If the outer wall of a disc breaks down completely and a disc fragment slips into the spinal canal, it’s called a herniated disc.
In addition, degeneration of the facet joints caused by osteoarthritis of the spine often leads to the development of bone spurs. These small, hard growths may protrude into the foramen or the spinal canal, constricting the exiting nerves or the spinal cord. Increased friction within joints may also irritate nearby ligaments, causing them to swell and take up more space in the spinal canal.
A facet joint can degenerate to such an extent that it no longer provides stability to the vertebra, which may slip out of place and move forward. In this condition, called spondylolisthesis, the vertebra can slip too far forward, putting pressure on the spinal cord or nerve roots.
Rarely, people are born with a narrow spinal canal or have a developmental condition that leads to a narrowing of the spinal canal. These include achondroplasia, scoliosis, and spina bifida, in which symptoms appear before age 50. Spinal stenosis may also be caused by a spine tumor.
A trauma to the spine, such as an injury from a car accident, that results in a dislocation or a fracture may also constrict nerves or the spinal cord at any point in the spine.”
Hmmm, I have degenerative disc disease and osteoarthritis of the spine. Add that to being a woman over the age of 50 and….
Now what? Let’s take a look at the symptoms, courtesy the Mayo Clinic:
“Spinal stenosis often causes no symptoms. When symptoms do occur, they start slowly and get worse over time. Symptoms depend on which part of the spine is affected.
In the lower back
Spinal stenosis in the lower back can cause pain or cramping in one or both legs. This happens when you stand for a long time or when you walk. Symptoms get better when you bend forward or sit. Some people also have back pain.
In the neck
Spinal stenosis in the neck can cause:
Numbness
Tingling or weakness in a hand, leg, foot or arm
Problems with walking and balance
Neck pain
Problems with the bowel or bladder”
Uh-oh, I neglected to mention that spinal stenosis can also occur in the neck.
Okay, here comes the part of the blog that deals with CKD. It’s in the treatment. While these are not the only treatments, they are the most often tried first. Healthline lays them out for us:
“There is no cure for spinal stenosis, but there are treatments to help relieve symptoms. Over-the-counter anti-inflammatory medications can ease swelling and pain. If they don’t do the trick, your doctor can prescribe higher-dose medication.
Your doctor may also recommend cortisone injections. This anti-inflammatory drug is injected directly into the area of the spinal stenosis. Cortisone can significantly ease inflammation and pain. Its effects may be temporary, however, and you shouldn’t have more than three injections in a single year.”
Marvelous, just marvelous. The OTC medications they’re referring to are NSAIDS. You know, the pain relief that our kidneys have adverse reactions to. The National Kidney Foundation reminds us:
“Many analgesics should not be used if there is decreased kidney function, because they reduce the blood flow to the kidney. “
Well, maybe something stronger? Cortisone? There’s a problem with that, too, if you have diabetes, the foremost cause of chronic kidney disease. My rheumatologist suggested we try one shot and see what happened to my blood sugar. What happened was almost textbook, according to VeryWellHealth:
“If you’re diagnosed with diabetes and receiving a cortisone injection, be aware of the potential for elevated blood sugars. Talk to your healthcare provider about the best way to manage this, as you may need to adjust your insulin dosage.
Remember these temporary elevations tend to resolve without treatment, but seek treatment if your blood sugars appear to be behaving in an extreme or unexpected manner.”
I don’t mean to mislead you. Physical therapy, exercise, weight loss, and the use of a cane and/or walker may also alleviate the pain. So, all is not lost even if you have CKD or diabetes along with spinal stenosis.
You can be immunocompromised without being a transplant. I know because I live with someone who is. Let’s just suppose he developed chronic kidney disease [Oh, no!]. Let’s see if this would further his CKD, or if his CKD would further the being immunocompromised.
We know that CKD is the progression of the decline of your kidney function for three months or more. Let’s go to my favorite dictionary yet again, the Merriam-Webster, for a definition of immunocompromised:
“having the immune system impaired or weakened (as by drugs or illness)”
Just in case the information is needed, let’s define the immune system, too.
“the bodily system that protects the body from foreign substances, cells, and tissues by producing the immune response and that includes especially the thymus, spleen, lymph nodes, special deposits of lymphoid tissue (as in the gastrointestinal tract and bone marrow), macrophages, lymphocytes including the B cells and T cells, and antibodies”
Well that certainly seems to cover it. Time to see what CKD and being immunocompromised have to do with each other, if anything. The National Institutes of Health starts us off on this exploratory journey:
“Impairment of the normal reaction of the innate and adaptive immune systems in chronic kidney disease predisposes patients to an increased risk of infections, virus-associated cancers, and a diminished vaccine response.”
You know, I’m not so sure I accepted that I’m immunocompromised before reading that. I feel more validated for still quarantining as much as possible and wearing a mask now. As usual, I want more information, so let’s find it.
“Cardiovascular disease and infections are directly or indirectly associated with an altered immune response, which leads to a high incidence of morbidity and mortality, and together, they account for up to 70% of all deaths among patients with chronic kidney dysfunction. Impairment of the normal reaction of the innate and adaptive immune systems in chronic kidney disease predisposes patients to an increased risk of infections, virus-associated cancers, and a diminished vaccine response.”
This bit of information from the National Library of Medicine surprised me. Not only does CKD affect being immunocompromised, but being immunocompromised affects your CKD.
“The immune system and the kidneys are closely linked. In health the kidneys contribute to immune homeostasis, while components of the immune system mediate many acute forms of renal disease and play a central role in progression of chronic kidney disease.”
We’re still not quite there. I want to know the mechanism of CKD causing us to be immunocompromised and vice-versa. I think I found the answer in Nature Reviews, but I’m not sure I understand it:
“The kidneys are frequently targeted by pathogenic immune responses against renal autoantigens or by local manifestations of systemic autoimmunity. Recent studies in rodent models and humans have uncovered several underlying mechanisms that can be used to explain the previously enigmatic immunopathology of many kidney diseases. These mechanisms include kidney-specific damage-associated molecular patterns that cause sterile inflammation, the crosstalk between renal dendritic cells and T cells, the development of kidney-targeting autoantibodies and molecular mimicry with microbial pathogens. Conversely, kidney failure affects general immunity, causing intestinal barrier dysfunction, systemic inflammation and immunodeficiency that contribute to the morbidity and mortality of patients with kidney disease.”
Hmm, maybe some definitions would help us understand. Let’s try that.
Pathogenic: specific causative agent (such as a bacterium or virus) of disease [Merriam-Webster Dictionary]
Autoantigens: Autoantigens are markers on cells inside your body that your immune system attacks even though they shouldn’t. Autoantigens cause autoimmune diseases. [Cleveland Clinic]
Sterile inflammation: Inflammation in the absence of pathogens and their products is referred to as sterile inflammation. [Annual Review]
Dendritic Cells: Dendritic cells are sentinels that constantly survey the kidney microenvironment for injury or infection; they recruit and regulate immune effector cells such as macrophages, T cells and neutrophils to protect the host. [Nature Reviews]
T-Cells: T cell, also called T lymphocyte, type of leukocyte (white blood cell) that is an essential part of the immune system. [Britannica]
Wow. That did work. I understand the mechanism now. Do you?
What would tip you off that you’re immunocompromised besides having CKD? Remember that CKD is not the only cause of being immunosuppressed. You probably want to keep an eye on other symptoms for those you care for. According to the Mayo Clinic:
“Frequent and recurrent pneumonia, bronchitis, sinus infections, ear infections, meningitis or skin infections
Inflammation and infection of internal organs
Blood disorders, such as low platelet count or anemia
Digestive problems, such as cramping, loss of appetite, nausea and diarrhea
Delayed growth and development
Autoimmune disorders, such as lupus, rheumatoid arthritis or type 1 diabetes”
CKD or not, you want to deal with that lack of immunity. VeryWellHealth has some advice that almost sounds like common sense to me:
“In general, it’s the cause of the immunodeficiency that’s treated, not the immunodeficiency itself. One treatment for immunodeficiency may be a bone marrow transplant. However, that’s only an appropriate treatment for individuals whose bone marrow isn’t producing enough immune cells.
When the immunodeficiency itself isn’t treatable, there are still other options. For example, there are therapies available that can help individuals fight off certain infections. You may also be more likely to need antibiotics or antiviral medications to fight diseases that immunocompetent people can ward off without treatment.”
You know what to do. You have chronic kidney disease. You need to treat it. Adhere to the kidney diet, get enough sleep, take your high blood pressure medication, exercise, avoid drinking, stop smoking, and keep yourself hydrated. The treatment for your immune deficiency is the same as the treatment for your CKD.
Here’s hoping you all realize that you are immunocompromised by virtue of having chronic kidney disease and treat yourself accordingly.
That’s been my refrain as a chronic kidney disease patient Stage 3 for the past 15 years. It made sense to me that dialysis patients might also be tired. But it simply hadn’t occurred to me that those with transplants might also feel fatigued. That is, until a reader asked why she was always so tired after her transplant.
Ah, I see you caught that I’m using tired and fatigued interchangeably. Let’s go over to my favorite dictionary, the Merriam Webster, for their definitions.
Tired “drained of strength and energy: fatigued often to the point of exhaustion”
Fatigued “drained of strength and energy “
Okay, now that we’ve established that they are synonymous, what do they have to do with those who had been transplanted? An article presented at the American Transplant Congress concluded:
“Fatigue is common in adults undergoing KT but improves over the first 7 months after transplantation. Additionally, live donor recipients tend to improve their fatigue scores faster than deceased donor recipients.”
KT is Kidney Transplantees.
But what about those who are still fatigued past the seven months mentioned above? Another article, this time on Lippincott Medicine, gives us some insight into how little is known:
“Fatigue is an extremely common symptom among kidney transplant recipients (KTRs), with prevalence ranging from 39% to 59%…. Fatigue can be described as an awareness of negative balance between available energy and the cost in physical, cognitive, emotional, or/and functional components. Patients with fatigue have more functional impairments and poorer quality of life…. However, it is often medically unexplained, clinically underestimated, and usually undertreated.”
We can’t stop here, leaving those who are fatigued after kidney transplantation hanging. Come to think of it, the same Lippincott article suggested that vitamin D may be helpful, but it’s not known why.
Another possible cause of this fatigue is diabetes. This is what England’s National Health Service has to say about diabetes and being tired after a kidney transplant:
“Diabetes is a common complication of having a kidney transplant.
Diabetes is a lifelong condition that causes a person’s blood sugar level to become too high. Some people develop it after a kidney transplant because, as they no longer feel unwell, they eat more and gain too much weight. Some types of immunosuppressants can also make you more likely to develop diabetes.
Symptoms of diabetes include:
feeling very thirsty
peeing a lot, especially at night
tiredness”
Or could it be depression and/or sleep disorders which cause the fatigue? The National Center for Biotechnology seems to think that could be true:
“Fatigue is a frequent and underestimated symptom of kidney transplant recipients. However, a significant lower rate of fatigue is observed in KTR patients compared with HD ones. The mechanisms underlying this symptom in KTR patients are essentially unknown. Fatigue is significantly associated with symptoms of depression and/or sleep disorders, is extremely debilitating and significantly impairs the quality of life while it remains unknown if it increases the risk of mortality. There is some evidence that fatigue may be improved by exercise.”
Remember the Lippincott article suggested vitamin D might be helpful? Now we have another possible avenue of improvement: exercise.
WebMD opened my eyes to the possible side effects of your anti-rejection medication:
“Here’s a general list of some of the side effects you might have:
Let’s take a good look at these. We already mentioned diabetes and trouble sleeping might contribute to the after kidney transplant fatigue. Nausea? Vomiting? Diarrhea? Have you ever had gastroenteritis [stomach flu]? Remember feeling like you just couldn’t move? That’s a cause of fatigue, too. The same with anemia. You’re tired beyond tired.
I’m sure you’re aware of my persistent use of possible and possibly in today’s blog. That’s because there’s not much known about the causes of long term fatigue after having had a kidney transplant. Then I wonder about fatigue itself as a cause of further fatigue. You’ve probably seen this transplant as a means to an end of your dialysis fatigue and now that hasn’t happened. Your depression about that may be a contributing factor.
A lot of this is conjecture on my part. We all know I’m not a doctor and don’t pretend to be. Now keep in mind that I’ve never had an organ transplant [ although I’ve had the opposite and am now missing my spleen, gall bladder, and ¾ of my pancreas!]. I’ve also never been on dialysis. So here you have the research I was able to unearth and my own speculation. I did want to mention that I discovered several studies suggesting that psychotherapy might be helpful.
Ugh! Another difficult blog to write that ended with no definitive findings. I suppose as a lay person, my best advice would be to explore each of the possible causes [and treatment of] long term fatigue after your kidney transplant with your transplant team. Here’s hoping I’ve given you enough information to open this particular conversation with them.
I was looking for some notes I’d made for today’s blog and couldn’t find them. Okay, so my office is being rearranged. After a few minutes of my kind of cursing [quite inventive, if I do say so myself], I accepted that I would just have to recreate them. Certainly not from memory since chemo brain and chronic kidney disease brain fog share the space in my brain. Yep, I was going to go back to the internet and research the topic all over again.
But I didn’t. I stumbled upon some information that blew me away. I had never wondered about this, not even a little. What is it, you ask. Let me answer your question with a question: Have you ever wondered how your kidneys came to be? That’s the information I stumbled upon, and it fascinated me. We’ll probably have to rely on quite a few definitions, but it’s still worth exploring. I’ll place the definitions in brackets next to the word being defined. They were gathered from my own brain and various sources.
The kidneys initially form near the tail of the embryo.
Vascular buds from the kidneys grow toward and invade the common iliac arteries [the ones that carry blood to the lower extremities].
Growth of the embryo in length causes the kidneys to ‘ascend’ to their final position in the lumbar [the lower spine and the part of the back near it] region.
Rather than ‘drag’ their blood supply with them as they ascend, the kidneys send out new and slightly more cranial [Of or relating to the skull or cranium] branches and then induce the regression of the more caudal [a. Of, at, or near the tail or hind parts; posterior: the caudal fin of a fish. b. Situated beneath or on the underside; inferior.] branches.
This is a highly regimented procedure. What if something goes awry? What could happen then? Back to Duke Medical for some possible answers:
“A. Duplication of the urinary tract
Occurs when the ureteric bud [what eventually becomes the ureter] prematurely divides before penetrating the metanephric blastema [the other part of the embryo that becomes part of the kidney, usually the nephrons].
Results in either a double kidney and/or a duplicated ureter and renal pelvis [“The renal pelvis is a chamber where all the urine-forming ducts meet and further routes urine to the urinary bladder.” Mansi Kohli.]
B. Renal-Coloboma syndrome
The Pax2 gene essential for metanephric mesenchyme [later to become nephrons, the filters in your mature kidneys] to differentiate into epithelial tubules [“Renal tubular epithelial cells are resident cells in the tubulointerstitium [connecting tissue between the cells in the tubules] that have been shown to play crucial roles in various acute and chronic kidney diseases.” National Library of Medicine.] in response to inductive signals from ureteric bud, so mutations (even if HETEROZYGOUS [Two variations of a gene on the same locus of a chromosome]) can produce renal defects. Patients typically exhibit the following symptoms:
Renal hypoplasia [incomplete development] – due to reduced proliferation of the mesenchyme [tissue found in organisms while they develop] derived epithelia [body tissue that covers all surfaces of your body, inside and out] during development.
Vesicouretral Reflux [Urine flows backwards up into the kidneys and ureters from the bladder] – most likely due to improper connection of the ureter to the bladder or possibly due to inherent defects in epithelial cells of the mature ureter.
Colobomas (ventral fissures in iris, retina, and/or optic nerve) – due to failure of the optic fissure to fuse (expression of Pax2 is observed in ventral part of the optic cup and optic stalk).
C. Nephroblastoma (Wilms Tumor)
found in infants from 0-24 months of age
consists of blastemal [a mass of cells that is capable of becoming an organ or appendage], epithelial, and stromal [supporting tissue] cell types
associated with mutations in genes related to kidney development (PAX2, WT1, etc.)
essentially due to incomplete mesenchymal-to-epithelial transformation (i.e. the cells fail to fully differentiate and transform into cancerous cells).
D. Polycystic kidney disease
can arise due to a variety of factors:
loss of polarity: aberrant differentiation of tubule cells results in inappropriate location of Na/K [sodium/potassium] channels to the apical [apex] (rather than basal [base]) domain of the cells. Na+ is pumped apically, water follows resulting in dilation of tubule lumens [part of the nephrons, have no red blood cells].
Overproliferation: excessive growth of tubule epithelium can occlude the lumen causing blockage.”
You have been incredible today reading a blog with all the definitions stuck in the descriptions. Thank you for bearing with me on that. I feel the mystery has been solved. I hope you do, too. Knowing how kidneys are formed, believe it or not, makes me feel more appreciative of them – even though I was already very appreciative of them.
With the holidays coming up, I’m going to be that nag who reminds you to take care of your kidneys. Watch your renal diet. Get adequate sleep. Try not to smoke or drink. Exercise even though you don’t want to. And most importantly of all, don’t let the stress get you. Avoid it, minimize it, do whatever you can to stay … without smoking or drinking.
The next blog will be on the 19th, which means it will be during Chanukah. Christmas and Kwanzaa won’t be far behind. Have I left out whatever holiday you observe? Let me know. Hmm, maybe next week’s blog should be about holiday meals.
Lately, everywhere I look I see some information about exercise. That’s probably because I’ve had enough of hiding from it. I didn’t feel like I had much control over my pancreatic cancer, but I did have control over whether I exercised or not. So, I didn’t. Bad move on my part. It’s taken me almost three years to understand that I wasn’t doing myself any favors by avoiding exercise.
So first, I tried tap dancing. I’d always wanted to learn how to do that. Gregory Hines was my hero at one time just because he was such a marvelous tap dancer. That didn’t work out too well. I have osteoarthritis in my feet, knees, and hips. My rheumatologist strongly suggested I NOT tap dance. Oh, well.
Then I thought I’d go back to walking. I used to love to take my dog on long, wandering walks. Unfortunately, Sweet Ms. Bella succumbed to her own cancer. A few years later, my big, fluffy, white dog, Shiloh, came to live with us. One thing this 70 lb. dog does not do is walk on a leash. That didn’t really matter as much as I’d thought it did because I got older and simply could no longer deal with the Arizona heat. I wonder if the chemotherapy had anything to do with that.
My third attempt at exercise was with an online app. This one was sort of a chair yoga. I hadn’t remembered about the bone on bone in my neck or the neuropathy in my hands and feet. Ouch! Not to worry, I’ll find something; it’s just a matter of trying.
Meanwhile, let’s take a look at why it’s so important for us to exercise. It’s important for everyone, but I mean chronic kidney disease patients and diabetes specifically.
‘I knew exercise was important to control my weight. It would also improve my blood pressure and lower my cholesterol and triglycerides. The greater your triglycerides, the greater the risk of increasing your creatinine. There were other benefits, too, although you didn’t have to have CKD to enjoy them: better sleep and improved muscle function and strength. But, as with everything else you do that might impinge upon your health, check with your doctor before you start exercising….
Keeping it simple, basically, there’s a compound released by voluntary muscle contraction. It tells the body to repair itself and grow stronger. The idea is to start exercising slowly and then intensify your activity….
What I didn’t know at the time is that your body becomes accustomed to a certain kind of exercise and then it isn’t as effective anymore….’”
I revisited the topic of exercise towards the end of last year and found new information, which makes sense since more than 10 years has passed since the publication of my first CKD book:
“As for lowering both parts of your blood pressure, that’s good news too since high blood pressure is the second most common cause of CKD …. By the way, systolic is the top number which measures your heart rate when blood is being pumped to all parts of your body. Diastolic is the bottom number which measure your heart rate when your heart is at rest.
Lowering your BMI is also a boon. Excess weight may lead to diabetes which, in turn, could lead to CKD. According to the National Center Biotechnology Information [NCBI],
‘A high body mass index is one of the strongest risk factors for new-onset CKD. In individuals affected by obesity, a compensatory hyperfiltration occurs to meet the heightened metabolic demands of the increased body weight. The increase in intraglomerular pressure can damage the kidneys and raise the risk of developing CKD in the long term.’”
And then, there’s the latest information about exercise from the National Kidney Foundation:
“How does exercise benefit me?
With exercise, it becomes easier to get around, do your necessary tasks and still have some energy left over for other activities you enjoy.
In addition to increased energy, other benefits from exercise may include:
Improved muscle physical functioning
Better blood pressure control
Improved muscle strength
Lowered level of blood fats (cholesterol and triglycerides)
Better sleep
Better control of body weight ….
Type of Exercise
Choose continuous activity such as walking, swimming, bicycling (indoors or out), skiing, aerobic dancing or any other activities in which you need to move large muscle groups continuously.
Low-level strengthening exercises may also be beneficial as part of your program. Design your program to use low weights and high repetitions, and avoid heavy lifting.
Work toward 30 minutes a session. You should build up gradually to this level.
There is nothing magical about 30 minutes. If you feel like walking 45 to 60 minutes, go ahead. Just be sure to follow the advice listed under “When should I stop exercising?” in this brochure.
How Often to Exercise
Exercise at least three days a week. These should be non-consecutive days, for example, Monday, Wednesday and Friday. Three days a week is the minimum requirement to achieve the benefits of your exercise.
How Hard to Work While Exercising
This is the most difficult to talk about without knowing your own exercise capacity. Usually, the following ideas are helpful:
Your breathing should not be so hard that you cannot talk with someone exercising with you. (Try to get an exercise partner such as a family member or a friend.) You should feel completely normal within one hour after exercising. (If not, slow down next time.)
You should not feel so much muscle soreness that it keeps you from exercising the next session.
The intensity should be a “comfortable push” level.
Start out slowly each session to warm up, then pick up your pace, then slow down again when you are about to finish.
The most important thing is to start slowly and progress gradually, allowing your body to adapt to the increased levels of activity.”
We’ve all heard that pets relax us. My family was a cat family until we moved into a house. We had so many dogs in Staten Island while the girls were growing up that I’m not sure I can remember them all. Here in Arizona, it’s only been my Sweet Ms. Bella – who instantly loved Bear – and Shiloh, our present big, fluffy, white dog.
Bella
I’m particularly interested in how our pets can help us with our chronic kidney disease. This all started when I wondered out loud what I should write about for this week’s blog. Bear called out, “Pets!” He was being silly, but I liked the idea. Let’s see if we can figure this out.
Here’s what the CDC has to say about having pets:
“There are many health benefits of owning a pet. They can increase opportunities to exercise, get outside, and socialize. Regular walking or playing with pets can decrease blood pressure, cholesterol levels, and triglyceride levels. Pets can help manage loneliness and depression by giving us companionship. Most households in the United States have at least one pet.
Studies have shown that the bond between people and their pets is linked to several health benefits, including:
Decreased blood pressure, cholesterol levels, triglyceride levels, feelings of loneliness, anxiety, and symptoms of PTSD.
Increased opportunities for exercise and outdoor activities; better cognitive function in older adults; and more opportunities to socialize”
Now, let’s apply that to CKD patients. Hypertension, or high blood pressure, is the second most common cause of chronic kidney disease. I turned to the National Institute of Diabetes and Digestive and Kidney Diseases [NIDDK) to pinpoint exactly how hypertension affects your kidneys:
“High blood pressure can constrict and narrow the blood vessels, which eventually damages and weakens them throughout the body, including in the kidneys. The narrowing reduces blood flow.
If your kidneys’ blood vessels are damaged, they may no longer work properly. When this happens, the kidneys are not able to remove all wastes and extra fluid from your body. Extra fluid in the blood vessels can raise your blood pressure even more, creating a dangerous cycle, and cause more damage leading to kidney failure.”
Thank you, Shiloh, with helping to keep my blood vessels unconstricted.
What about high cholesterol levels? WebMD was able to help us out here:
“Cholesterol is a waxy substance. Your body makes it and uses it to build your cells. You also get it from many foods. But having too much cholesterol can lead to health problems….
High cholesterol can build up in arteries to increase your risk of a heart attack or stroke. It turns out that high cholesterol isn’t good for your kidneys either.”
Along with high cholesterol, high triglycerides are detrimental to your kidneys. These fats in your blood can lead to diabetes, which is the foremost cause of CKD. High triglycerides might also raise your creatinine level. You need to remember that you do need some triglyceride since they store unused calories. These are used by your body for energy. You just don’t want high triglycerides.
I had no idea my dogs and cats were helping me control my CKD. By the way, other pets can also help. It doesn’t have to be a dog or cat.
We know – fortunately or not – that exercise if important if you have CKD. This is something I explored in my first CKD book: What Is It and How Did I Get It? Early Stage Chronic Kidney Disease:
“I knew exercise was important to control my weight. It would also improve my blood pressure and lower my cholesterol and triglyceride s. The greater your triglycerides, the greater the risk of increasing your creatinine. There were other benefits, too, although you didn’t have to have CKD to enjoy them: better sleep and improved muscle function and strength. But, as with everything else you do that might impinge upon your health, check with your doctor before you start exercising….
Keeping it simple, basically, there’s a compound released by voluntary muscle contraction. It tells the body to repair itself and grow stronger. The idea is to start exercising slowly and then intensify your activity….
What I didn’t know at the time is that your body becomes accustomed to a certain kind of exercise and then it isn’t as effective anymore.”
I can’t walk Shiloh since she ends up walking me, but we play. We run back and forth down the length of the long central hallway in the house. I’m certain you can figure out how to get some exercise playing with your pet if you, too, cannot walk him.
Shiloh
As an older adult, I was interested in the “better cognitive function in older adults” benefit of having a pet. As a CKD patient, I wondered if it would have any effect on CKD brain fog. The National Center For Biotechnology Information [NCBI) succinctly tells us via their work that not nothings been proven about this yet:
“Exercise interventions are likely to be beneficial based on biological plausibility and pilot trial data.”
Relaxation is also helpful if you have CKD. Stress needs to be avoided. Petting your pet or otherwise spending time with them is relaxing. Avoiding stress is one of the ways you could help delay the worsening of your chronic kidney disease.
I like to rub behind Shiloh’s ears. She loves it and it relaxes me. I also like to brush her. She leans into the brush, and I baby talk to her. Both of us benefit from this form of relaxation. Bear likes to rub her belly. Again, they both love it… and I’ll bet they’re both benefiting from this.
All on Amazon
Yes, I do think pets help in dealing with your CKD. Who couldn’t use lowered blood pressure, cholesterol, triglycerides, and a chance at extra stress relief? Do you have a pet? IF not, would you consider getting one after reading this blog?
Those of us with CKD always say that, don’t we? There’s so much we have to change about our lives once we’re diagnosed. That is, if you want to keep your CKD under control and possibly slow down its progression. There are the dietary changes to start. Then the medications. Don’t forget the lifestyle changes: exercise, avoid alcohol, no drinking, rest, adequate sleep. We all know the drill.
However, those are not the only things that changed in my life. I’d written ‘how to’s, literary guides, and study guides for decades. I’d taught research writing on the college level… and I’d earned an Academic Certificate in Creative Writing. Add my having been a teacher for most of my adult life and you have the basis for a CKD awareness advocate. That is how my life changed the most with my diagnosis.
The first thing I did was research for myself. I then decided that was pretty selfish. What about the people who didn’t understand what their nephrologists were saying and didn’t know how to research for themselves? Keep in mind, this was back in 2008 way before the patient based treatment movement began.
I had never published a book myself. Rather, I had always written for publishers at their request. That changed with my desire to become an advocate for CKD awareness. My thinking was, “Who’s going to publish a book about CKD for patients by a lay person?” I was and I did. What Is It and How Did I Get it? Early Stage Chronic Kidney Disease was the first book. I kept it reader friendly and explained what I hadn’t understood and what others had asked me about.
That sparked a bunch of readings at bookstores, coffee shops, and civic clubs. Then the book was mentioned in various publications, both locally and nationally. I was getting the word out! The book and its information also ignited requests from various groups for articles and/or caused those groups I’d requested to write for to change their minds and say yes. I even organized a Kidney Walk out here in Arizona. And now I serve as a patient advisor for two pharmaceutical companies.
What struck me the most was when an Indian doctor told me about how very poor his patients were and that he wanted them to have the information in the book, but they couldn’t possibly afford it. Together, we worked out a plan for me to blog a chapter a week. He would print each week’s blog and make multiple copies for his patients. Great! Now I just needed to learn how to blog.
Again, I did… with the help of my older daughter. Thank goodness she knew what she was doing because I didn’t. But it worked. I blogged as SlowItDownCKD. Once the books’ chapters were all blogged, I was having such fun being a CKD awareness advocate that I didn’t want to stop. So, I didn’t and that’s where the SlowItDownCKD book series began. Each year I would gather that year’s blogs and format them into a book. At this point, they go from 2011 to 2021.
You’re right; no once can keep covering the basics of CKD for a decade. I branched out into writing about dialysis, transplant, pediatric nephrology, and different kinds of kidney disease. There were also guest blogs from the adult children of CKD patients, transplantees, other CKD writers, and innovators.
I no longer give book talks or participate in meetings, unless they are online. Covid and cancer took my energy. But I still write and will continue to do so. I still feel it’s important that people know about this disease. So many have CKD and don’t know it. It’s sort of sad since all it takes is a blood test and a urine test to be diagnosed. I urge you to keep telling your friends and family how easy it is to make certain they’re not part of the club no one wants to join. Thanks for taking the time to read my story.
And thanks to all the readers who share the blog, talk to others about it, buy the books and share them with friends and family. Thanks to all those who urge their friends and family to get tested, who go with them to be tested, and who accompany them to be an extra ear at their nephrology appointments. And thanks to those who urge their nephrologists to remember to explain and ask questions of their patients.
According to the Centers for Disease Control and Prevention (CKD):
“More than 1 in 7, that is 15% of US adults or 37 million people, are estimated to have CKD. As many as 9 in 10 adults with CKD do not know they have CKD. About 2 in 5 adults with severe CKD do not know they have CKD.”
That is as of last year and only for the United States. I turned to MedAlertHelp to find the global statistics:
“The global estimated CKD prevalence is between 11.7% and 15.1%. To be more specific, that’s around 13.4%, or 850 million people suffering from chronic kidney disease worldwide, as per chronic kidney disease statistics worldwide for 2020….”
That was two years ago. Imagine what it is now. Surely, you can see the need for CKD awareness. You can help. Start talking about chronic kidney disease… please.
We all have water guidelines. Those on dialysis need to keep it down and those who aren’t need to keep it up. For example, my nephrologist suggested 64 ounces per day. That’s the equivalent of eight glasses of eight ounces each. To be honest, I use a water bottle that has the ounces marked on it. It’s just easier.
Yet, eight ounces is not right for everyone. The National Kidney Foundation makes several recommendations: men usually need about 13 ounces while women need nine; and using their own words:
“A common misconception is that everyone should drink eight glasses of water per day, but since everyone is different, daily water needs will vary by person. How much water you need is based on differences in age, climate, exercise intensity, as well as states of pregnancy, breastfeeding, and illness.”
“Water helps your kidneys remove waste from your blood. Your body excretes these wastes and excess fluids in the form of urine that travels to your bladder before leaving your body. Water also helps keep your arteries open so that your blood can flow freely to your kidneys. This blood delivers oxygen and nutrients that help your kidneys function. Dehydration makes it more difficult for this delivery system to work.
Mild dehydration can impair normal bodily functions, including your kidneys. Severe dehydration can actually lead to kidney damage. Drinking fluids is the best way to avoid dehydration, especially when you work or exercise especially hard or in warm or humid weather.
People with diabetes, kidney disease or other illnesses that affect the kidneys need to take in adequate amounts of fluid to keep their kidneys performing well. People with low blood pressure need to take in plenty of fluids to maintain kidney health, for example. Your kidneys act like filters to remove toxins from your body. To push blood through the filters, though, the blood has to be moving with force; in cases of low blood pressure, there is not enough pressure to force the blood through the tiny filters of the kidneys.”
Notice, please that the word ‘water’ has been replaced by the word ‘fluid.’
But wait a minute, I drink two eight-ounce cups of black coffee most every day. Coffee is mostly water, isn’t it? Does that count in my water – or fluid – allowance? Let’s figure it out. I went to Everyday Health for this information:
“There are so many different types of coffee to choose from, and your personal preference will affect how much hydration you’ll get from your brew. Two main factors dictate how much hydration you’ll be getting: the amount of caffeine and the volume of the beverage. For example, according to Mayo Clinic, an 8-oz cup of regular brewed coffee contains about 96 mg of caffeine while the same sized cup of decaffeinated brewed coffee contains only 2 mg of caffeine. This means, while you’ll be getting about 7 oz of hydration from the regular coffee, you’ll be getting the full 8 oz of fluid from the decaf. Caffeinated instant coffee falls somewhere in between, with 62 mg of caffeine per 8-oz serving. Similarly, a 1-oz serving of espresso contains about 64 mg of caffeine, which gives it almost as much diuretic power as a full 8 oz of caffeinated coffee, but since that’s all packed into only 1 oz of fluid, you’re really not getting any hydration from a shot of espresso.”
Wow! That means I’m getting 14 of my 64 ounces from my favorite beverage. I only drink water and the black coffee, but if I’m ill or having stomach problems, I will eat soup. Is that a fluid, too?
My favorite dictionary, the Merriam-Webster, defines soup for us:
“a liquid food especially with a meat, fish, or vegetable stock as a base and often containing pieces of solid food”
Double wow! So even if I’m not that hungry and just have a cup of soup, there’s another eight ounces or so of liquid, or as I see it being called now, hydration. So now I’ve had about 24 of my 64 ounces of liquid [no longer just water and sometimes called hydration] requirement for the day.
Hmmm, if soup counts as a liquid and coffee counts as a liquid [tea, too], what else does? Thanks to the American Kidney Fund’s Kidney Kitchen for the following graphic:
“Examplesof fluid:
Ice
Soups and stews
Pudding
Ice cream, sherbet, sorbet, popsicles, etc.
Protein drinks (Nepro, Novasource, Ensure, etc.)
All beverages (water, soda, tea, coffee, milk, nondairy milk, etc.)
Jell-O® other gelatin products and gelatin substitutes (pectin, arrowroot powder, etc.)”
Triple wow! So, if you get tired of water, water, water [I don’t.] to fulfill your fluid or hydration needs, look at the variety of foods you can have. Of course, if you have diabetes, you’d have to get the sugar free versions of these foods… and, please, no chemical artificial sweeteners. Sort of opens up the world of fluids, doesn’t it? [Notice I’m using the word ‘fluids’ or the word ‘hydration’ instead of the word ‘water.”]
“Fluid is a liquid or any food that turns into a liquid at room temperature…. Fruits and vegetables naturally contain water. If consumed in moderation, fruits and vegetables should not contribute large volumes of water to your daily total intake of fluids. Therefore, fruits and vegetables do not need to be counted as part of your daily fluid intake.”
I prefer to stick with my water and coffee but look at all the foods that have been made available to you. My favorite treat as a child was chocolate pudding. I remember the smooth, rich creaminess of it. My brother’s was orange jello. He said it felt cool going down his throat. I’ll be content with my memories. You go enjoy these foods.
World Kidney Day was March 10th this year. While I publicized it widely on social media, I didn’t blog about it because I have just about every year for the last 11 years or so. Just scroll to ‘World Kidney Day’ on the topics dropdown to the right of the blog and you can read last year’s blog about it.
By now, we all know March is National Kidney Month as well as Women’s History Month. Did you know it’s also National Nutrition Month? National Day Calendar tells us there is much more being celebrated this month:
“Asset Management Awareness Month
Developmental Disabilities Awareness Month
Endometriosis Awareness Month
Irish-American Heritage Month
Multiple Sclerosis Awareness Month
National Athletic Training Month
National Brain Injury Awareness Month
National Breast Implant Awareness Month
National Caffeine Awareness Month
National Celery Month
National Cerebral Palsy Awareness Month
National Cheerleading Safety Month
National Craft Month
National Colorectal Cancer Awareness Month
National Credit Education Month
National Flour Month
National Frozen Food Month
National Kidney Month
National Noodle Month
National Nutrition Month
National Peanut Month
National Sauce Month
National Trisomy Awareness Month
National Umbrella Month
National Women’s History Month
National Social Work Month”
I’ll admit I had to look up Trisomy. I figured it was three something since tri means three. The Medical Dictionary backed me up:
“the presence of an additional (third) chromosome of one type in an otherwise diploid cell (2n +1).”
Now, I’ll agree with you that some of these seem pretty silly, but I also think it’s no accident that National Kidney Month and National Nutrition Month are both in March. Wait, before I forget, you can also use the topic dropdown to read last year’s blog on National Women’s History Month.
Your body needs protein to help build muscle, repair tissue, and fight infection. If you have kidney disease, you may need to watch how much protein you eat. Having too much protein can cause waste to build up in your blood, and your kidneys may not be able to remove all the extra waste. If protein intake is too low, however, it may cause other problems so it is essential to eat the right amount each day.
The amount of protein you need is based on:
your body size
your kidney problem
the amount of protein in your urine
Your dietitian or healthcare provider can tell you how much protein you should eat.”
My first nephrologist limited me to 5 ounces of protein daily 13 years ago. That still hasn’t changed.
What about that one S? I thought the National Kidney Fund would be helpful here and they were, as long as you remember sodium, the 1 S, is one of the two elements of table salt:
“Salt makes you thirsty and can make your body retain fluid. Having more fluid in your body can raise your blood pressure. When you have high blood pressure, your kidneys must work harder to filter blood. Over time, this can lead to kidney damage.
Too much fluid in your body also puts more strain on your heart, lowers your protein levels, and leads to difficulty breathing. Taking steps to limit excess fluid buildup, and thereby controlling blood pressure, is vital to improving your health.
If you have high blood pressure, eating a low or no added salt diet can help to lower it. Increasing your daily physical activity and taking blood pressure medicines if prescribed by your doctor are other ways to manage your blood pressure. Taking steps to keep your blood pressure at a healthy level may help keep kidney disease from getting worse.”
2 Ps to go. One of them is potassium. I went right to my old and trusted site WebMD for information:
“Every time you eat a banana or a baked potato with the skin on (not just the tasty buttered insides), you’re getting potassium. This essential mineral keeps your muscles healthy and your heartbeat and blood pressure steady.
If you have a heart or kidney condition, though, your doctor may recommend a low-potassium diet. Your kidneys are responsible for keeping a healthy amount of potassium in your body. If they’re not working right, you may get too much or too little.
If you have too much potassium in your blood, it can cause cardiac arrest — when your heart suddenly stops beating.
If you have too little potassium in your blood, it can cause an irregular heartbeat. Your muscles may also feel weak.”
Hang on, here’s the last P – phosphorous. That’s the one element you usually don’t find on food labels. For CKD patients, that’s pretty annoying since you may have to keep track of all 3 Ps and 1S at your nephrologist’s or renal dietitian’s direction. Mayo Clinic, another trusted site I’ve been consulting for over a dozen years, explains:
“Phosphorus is a mineral that’s found naturally in many foods and also added to many processed foods. When you eat foods that have phosphorus in them, most of the phosphorus goes into your blood. Healthy kidneys remove extra phosphorus from the blood.
If your kidneys don’t work well, you can develop a high phosphorus level in your blood, putting you at greater risk of heart disease, weak bones, joint pain and even death ….
How much phosphorus you need depends on your kidney function. If you have early-stage kidney disease or you’re on dialysis, you may need to limit phosphorus. Nearly every food contains some phosphorus, so this can be hard to do.”
While National Nutrition Month is for everyone, we – as CKD patients – need to pay more than usual attention to our nutrition if we don’t want our chronic kidney disease to go spiraling out of control. Naturally, our diets need to be individualized based on the stage of our disease and diet is not all there is to slowing down the progression of the decline of your kidney function (the definition of CKD), but it’s a start.
For the last two years I’ve been grappling with exercise. I know it’s necessary, but I don’t want to do it. I keep telling myself that I’ll get over it; it being my need for control ever since I had cancer. I couldn’t control that, but I could control whether or not I exercised. I know it’s more than a little bit ridiculous, but the emotions don’t always listen to logic. Over a decade ago I wrote my first chronic kidney disease book: What Is It and How Did I Get It? Early Stage Chronic Kidney Disease. I included a chapter on exercise. Maybe that would help. I didn’t want to copy the entire chapter for today’s blog, so here you have what I consider the relevant parts. Maybe it’ll help you, too, if you’re having the same problem as I am. I know from reader comments that many of us are in the same exercise boat. Ready? Let’s start rowing.
“I knew exercise was important to control my weight. It would also improve my blood pressure and lower my cholesterol and triglyceride levels. The greater your triglycerides, the greater the risk of increasing your creatinine. There were other benefits, too, although you didn’t have to have CKD to enjoy them: better sleep, and improved muscle function and strength. But, as with everything else you do that might impinge upon your health, check with your doctor before you start exercising.
I researched, researched, and researched again. Each explanation of what exercise does for the body was more complicated than the last one I read. Keeping it simple, basically, there’s a compound released by voluntary muscle contraction. It tells the body to repair itself and grow stronger. The idea is to start exercising slowly and then intensity your activity….
I’ve discovered articles that say you need to exercise every day, and those that say you need to take a day or two off each week. Frankly, I’m at the point where I try for every day but remember the articles that say take a day or two off each week if I don’t get to make the time every day that week. I don’t know if it’s a function of age or not, but sometimes the day slips away, and I haven’t exercised yet.
For me, planning is important. For example, I’m going dancing tonight, [Update: Covid put an end to that.] so I know I don’t have to stop writing to exercise. Yesterday, I did – so I figured that since I can’t sit still at the computer for more than two hours at a time, I’d use the exercise bike [Update: long gone in deference to my knees and hip] and watch a movie during my second computer break. The day before, I had appointments left and right without too much time for myself, so I had my coffee in the morning then used a one mile walking tape. I usually use a three mile tape, but knew time was going to be tight that day and figured one mile was better than no miles….
There are days when an arthritic hip prevents me from doing any full body exercise. I make sure no one is watching, then I dance vigorously but only from the waist up. If it’s summertime here, I can water walk without too much pain when the arthritis acts up. [Update: Covid ended that, too.]
The point is that exercise is going to help you impede the progress of your CKD. Learn to at least tolerate exercise, if you can’t learn to love it.”
This was written over 11 years ago and seems a bit simplistic. Let’s see what newer information there is about exercise and ckd. BMC, a research publisher, included a 2019 study by BMC Nephrologywhich concluded:
“…exercise therapy may be a potential strategy to improve eGFR, reduce SBP, DBP and BMI in non-dialysis CKD patients. Limited evidence from short-term studies suggests that exercise may reduce TG, but not Scr, TC, HDL or LDL.”
Don’t worry. They also included definitions for the abbreviations:
“SBP: Systolic blood pressure
DBP: Diastolic blood pressure
BMI: Body mass index
TG: Triglyceride
SCr: Serum creatinine
TC: Total cholesterol
HDL: High density lipoprotein
LDL: Low density lipoprotein”
This sounds suspiciously like the list of what exercise can do for anyone, not just ckd patients, except for one very important aspect: eGFR. That’s your estimated glomerular filtration rate. In other words, it’s the evaluator of your kidney health. The higher the function, the better your kidneys are working.
My eGFR just tanked to 40, almost the lowest it’s ever been. It’s probably due to using two different kinds of insulin, but that’s a blog for another day. The point is that exercise became part of my daily routine as soon as I saw that blood test result. Enough of these emotive issues. Time to return to logic.
As for lowering both parts of your blood pressure, that’s good news too since high blood pressure is the second most common cause of ckd here in the USA. By the way, systolic is the top number which measures your heart rate when blood is being pumped to all parts of your body. Diastolic is the bottom number which measure your heart rate when your heart is at rest.
Lowering your BMI is also a boon. Excess weight may lead to diabetes which, in turn, could lead to ckd. According to the NCBI [National Center for Biotechnology Information],
“A high body mass index is one of the strongest risk factors for new-onset CKD. In individuals affected by obesity, a compensatory hyperfiltration occurs to meet the heightened metabolic demands of the increased body weight. The increase in intraglomerular pressure can damage the kidneys and raise the risk of developing CKD in the long term.”
Got it. Let’s both get off the computer and get moving.
My husband suffers from tinnitus and often complains about how loud “the crickets” are. He tells me there’s nothing that can be done about this. But then, a reader asked about tinnitus, and I realized chronic kidney disease patients have a three time more likelihood of developing this malady. Now I can no longer accept that nothing can be done.
Let’s start at the beginning. Just what is this? Oh goody, time to consult my favorite dictionary. That, of course, is The Merriam-Webster:
“a sensation of noise (such as a ringing or roaring) that is typically caused by a bodily condition (such as a disturbance of the auditory nerve or wax in the ear) and usually is of the subjective form which can only be heard by the one affected”
Wait a minute. That doesn’t say anything about chronic kidney disease. But a large study published by The National Center for Biotechnology Information [(NCBI] does:
“This study presented that CKD is a significant and independent risk factor for tinnitus. The patients with CKD have a 3.02 times higher risk of developing tinnitus. Furthermore the patients with end stage renal disease and dialysis are at a 4.586 times risk of tinnitus than general population and carry a higher risk of tinnitus than the patients with CKD and without dialysis….”
The NCBI is part of the United States National Library of Medicine [NLM], which is a branch of the National Institutes of Health [NIH].
Everyday Health tells us what the causes of tinnitus may be:
“Tinnitus is often associated with high blood pressure, allergies, and abnormal kidney function. Tinnitus can also occur because of:
Tumors
Cardiovascular problems
Medication side effects
Loss of hearing
Being around very loud noises
A head or neck injury
Bones in the middle ear that become harder”
Did you notice “high blood pressure” and “abnormal kidney function” in the explanation above? By the way, my husband had been around very loud noises the whole time he served in Vietnam.
I found a highly readable explanation on the connection between the kidneys and ears at Hearing Unlimited.
“If you asked a medical professional about the kidneys and the ears, they would tell you that ‘the kidneys share physiologic, ultrastructural and antigenic similarities with the stria vascularis of the cochlea.’ Or, in plain English: a specific part of our ears shares functional and structural characteristics with our kidneys.
It almost sounds unreal – how could the ears share similarities with the kidneys? But research has confirmed that physiological mechanisms of fluid and electrolyte balance are present in both organs. This matters because it means that when a health issue affects the functionality of one (i.e. the kidneys or the ears), it’s likely to affect the other ….”
Now what? It’s there. You have CKD, but you don’t know if that’s the cause of your tinnitus. WebMD has some suggestions that may or may not work, but they seem worth a try… except for those you just can’t try because you have CKD. For example, I’d stay away from the herbals because they aren’t regulated. Do check any other medications with your nephrologist before you proceed.
“Even if a specific cause is never found, there is still hope for successful treatment. A combination of therapies over time usually offer the best hope.
Biofeedback, relaxation training, counseling, and individualized psychotherapy helps manage stress and helps you change your body’s reaction to the tinnitus. Tinnitus Retraining Therapy (TRT) combines counseling with special background sounds designed to help people suppress the sounds of their tinnitus.
Antianxiety medications, such as Valium or Xanax, as well as a wide range of antidepressant medications, are very helpful for tinnitus sufferers. Other medications, such as diuretics (water pills), muscle relaxants, anticonvulsants medications, and antihistamines, are also used.
Special hearing aids, electronic masking devices, or both, are often used when other methods have failed to achieve control. Cochlear implants and cochlear stimulation devices are being investigated for severe, intractable tinnitus cases. Surgical injections of lidocaine directly into the inner ear are also being used in some cases.
Alternative treatments such as hypnosis, acupuncture, chiropractic adjustments, vitamin/mineral supplements, and herbal remedies may have some promise, but there is little, if any, meaningful research as to their effectiveness. Ginkgo biloba — which is being studied to determine its effectiveness for tinnitus — is said to improve blood flow and nerve function. Use ginkgo biloba with caution if you have a bleeding disorder or take blood thinners. Explore alternative options carefully, with the cooperation of your medical providers.”
That got me to wondering if lifestyle changes could be of any help. Bingo! Hearing Associates of Las Vegas suggests you avoid the following:
Avoiding smoking and drinking more water are two suggestions that would help your CKD even if you didn’t have tinnitus.
I got curious about the special hearing aids since that’s something we hadn’t tried for my husband. In attempting to research that, I discovered something called a masker.
“A tinnitus Masker is an electronic hearing aid device that generates and emits broad-band or narrow-band noise at low levels, designed to mask the presence of tinnitus.
Such masking noise is also referred to as white noise. For an individual suffering from both hearing loss and tinnitus, the masker and the hearing aid can operate together as one instrument.”
This information is from Hear-It. I thought you might think they were a selling site [as I did], so I’m including this information from their website:
“Hear-it.org is a non-commercial web site and has been established to increase public awareness of hearing loss. Hear-it.org is one of the world’s leading and most comprehensive websites on hearing, hearing loss and tinnitus and how to treat and live with hearing loss or tinnitus.”
With Mother’s Day last month and Father’s Day this month, I’ve been thinking about family a lot. Basically, I’ve been wondering if there are any oblique links to chronic kidney disease for any members of my family. As I ruminated, one link popped up. One of my daughters has PCOS… and has recently been diagnosed with diabetes… which we know is the primary cause of CKD. Uh-oh.
Let’s see how this all works. We know that CKD is the progressive decline of your kidney function for at least three months. We know that diabetes is either not producing insulin, which is type 1, or being unable to make use of the insulin you do produce, which is type 2. By the way, I’m type 2 but that was diagnosed many years after the ckd was diagnosed for me. CKD is also a prime cause of diabetes. It works both ways: CKD can cause diabetes and diabetes can cause CKD.
And PCOS? Each time, my daughter tells me about it I have to ask, “Uh, what is that again?” PCOS is polycystic ovary syndrome. Big help, huh? Thank goodness for a more thorough answer from my old buddy TheMayoClinic:
“Polycystic ovary syndrome (PCOS) is a hormonal disorder common among women of reproductive age. Women with PCOS may have infrequent or prolonged menstrual periods or excess male hormone (androgen) levels. The ovaries may develop numerous small collections of fluid (follicles) and fail to regularly release eggs.
The exact cause of PCOS is unknown. Early diagnosis and treatment along with weight loss may reduce the risk of long-term complications such as type 2 diabetes and heart disease.”
I wondered if my daughter knew something was amiss or if her doctor picked this up, so I did the usual – looked up the symptoms. I found John Hopkins Medicine the most helpful source for this information:
“The symptoms of PCOS may include:
Missed periods, irregular periods, or very light periods
Ovaries that are large or have many cysts
Excess body hair, including the chest, stomach, and back (hirsutism)
Weight gain, especially around the belly (abdomen)
Acne or oily skin
Male-pattern baldness or thinning hair
Infertility
Small pieces of excess skin on the neck or armpits (skin tags)
Dark or thick skin patches on the back of the neck, in the armpits, and under the breasts”
Wait a minute. This is not that clear. Where does the insulin part of PCOS come in? That’s what is responsible for diabetes and diabetes is the foremost cause of CKD. Webmd explains:
“Your body makes hormones to make different things happen. Some affect your menstrual cycle and are tied to your ability to have a baby. The hormones that play a role in PCOS include:
Androgens. They’re often called male hormones, but women have them, too. Women with PCOS tend to have higher levels.
Insulin. This hormone manages your blood sugar. If you have PCOS, your body might not react to insulin the way it should.
Progesterone. With PCOS, your body may not have enough of this hormone. You might miss your periods for a long time or have trouble predicting when they’ll come.”
Aha! So PCOS interferes with your insulin… which is practically the definition of insulin. MedicalNewsToday confirms this in describing the three major types of diabetes:
“Type I diabetes: Also known as juvenile diabetes, this type occurs when the body fails to produce insulin. People with type I diabetes are insulin-dependent, which means they must take artificial insulin daily to stay alive.
Type 2 diabetes: Type 2 diabetes affects the way the body uses insulin. While the body still makes insulin, unlike in type I, the cells in the body do not respond to it as effectively as they once did. This is the most common type of diabetes, according to the National Institute of Diabetes and Digestive and Kidney Diseases, and it has strong links with obesity.
Gestational diabetes: This type occurs in women during pregnancy when the body can become less sensitive to insulin. Gestational diabetes does not occur in all women and usually resolves after giving birth.”
Let’s move on to how diabetes can cause CKD, just in case you’ve forgotten. The National Institutes of Diabetes and Digestive and Kidney Diseases, which is part of the National Institutes of Health, which is part of the U.S. Department of Health and Human Services is of service here:
“High blood glucose, also called blood sugar, can damage the blood vessels in your kidneys. When the blood vessels are damaged, they don’t work as well. Many people with diabetes also develop high blood pressure, which can also damage your kidneys….”
Remember, it’s your insulin that controls the amount of blood glucose you have. Without producing insulin or if your body doesn’t respond well to insulin, you have diabetes. If you have diabetes your kidneys’ blood vessels may be damaged and you may ‘develop high blood pressure,’ which is a major cause of CKD.
High blood pressure is actually the second most likely cause of CKD. So, it seems that PCOS can lead to diabetes which may lead to high blood pressure, the latter two both major causes of CKD. It seems to me that I noticed cardiovascular risk can also be associated with PCOS. VeryWellHealth makes it clear how this happens:
“Having PCOS increases a woman’s chances of getting heart-related complications.
This is due to the higher levels of insulin that have been associated with PCOS and are known to increase one’s risk for elevated triglycerides, low levels of high-density lipoprotein (HDL), high cholesterol, blood pressure, and atherosclerosis. These conditions can increase your risk for a heart attack and stroke.”
I wonder if you’ve realized that CKD can also cause heart problems. The Kidney Fund clarifies:
“The heart and the kidneys work closely together. When there is a problem with one, things can go wrong in the other. Heart disease can cause CKD, and CKD can also cause heart disease.
When you have heart disease, your heart may not pump blood in the right way. Your heart may become too full of blood. This causes pressure to build in the main vein connected to your kidneys, which may lead to a blockage and a reduced supply of oxygen rich blood to the kidneys. This can lead to kidney disease.
When the kidneys are not working well, your hormone system, which regulates blood pressure, has to work harder to increase blood supply to the kidneys. When this happens, your heart has to pump harder, which can lead to heart disease.”
It is all connected. PCOS to diabetes to CKD to heart problems. Before you start to worry, it doesn’t have to be like that. Take care of yourself and prevent the diseases if you can.
The world has acknowledged World Kidney Day. We have had walks in many countries. We have had educational seminars in many countries. We have posted in many countries. All to bring awareness to what our kidneys do for us and the worldwide challenge of kidney disease. Thursday, March 11th, was World Kidney Day.
But today is Monday. And you know what? It’s still March, National Kidney Month, here in the United States. Each year, I write about National Kidney Month, just as I write about World Kidney Day. Interesting tidbit: the Philippines also has a National Kidney Month which they celebrate in June. I’ll only be writing about the U.S.’s National Kidney Day.
As usual, let’s start at the beginning. What is National Kidney Month? Personalized Cause has a succinct explanation for us. While I’m not endorsing them since I usually try to avoid endorsements, I do want to let you know they sell the green ribbons and wristbands for kidney disease awareness that you’ll probably be seeing hither and yon all month.
“National Kidney Month, observed in March and sponsored by the National Kidney Foundation, is a time to increase awareness of kidney disease, promote the need for a cure, and spur advocacy on behalf of those suffering with the emotional, financial and physical burden of kidney disease. The National Kidney Foundation is the leading organization in the U.S. dedicated to the awareness, prevention and treatment of kidney disease for hundreds of thousands of healthcare professionals, millions of patients and their families, and tens of millions of Americans at risk.
National Kidney Month is a time to increase awareness about the function of the kidneys and kidney disease. Kidneys filter 200 liters of blood a day, help regulate blood pressure and direct red blood cell production. But they are also prone to disease. One in three Americans is at risk for kidney disease due to diabetes, high blood pressure or a family history of kidney failure. There are more than 26 million Americans who already have kidney disease, and most do not know it because there are often no symptoms until the disease has progressed.”
That, of course, prompted me to go directly to the National Kidney Foundation’s information about National Kidney Month. This is what I found:
“March 1, 2021, New York, NY — In honor of National Kidney Month which starts today, the National Kidney Foundation’s (NKF) national public awareness campaign, “Are You the 33%?” enters a new phase focusing on the connection between type 2 diabetes (T2D) and kidney disease, also known as chronic kidney disease (CKD). NKF urges everyone to find out if they’re the 1 in 3 at risk for developing kidney disease by taking a one-minute quiz at MinuteForYourKidneys.org.
Diabetes is a leading risk factor for developing kidney disease. Over time, having high blood sugar from diabetes can cause damage inside your kidneys. But it doesn’t have to end up this way; because with careful control of glucose (sugar) levels, there is evidence that you can prevent kidney disease in people with diabetes.
Award-winning actress, Debbie Allen joined the campaign as the T2D Campaign Celebrity Spokesperson in February, Black History Month, to help promote awareness of diabetes as a leading cause for developing chronic kidney disease. Allen has a family history of diabetes and was recently diagnosed with pre-diabetes.”
Indeed, the National Kidney Foundation has a lot to offer with peer mentoring, community, an information helpline, and transplant, palliative care, dialysis, kidney donation, and research information.
The American Kidney Fund [AFK] joins in National Kidney Month with their form to pledge to fight kidney disease. I signed up; you can, too, if you’d like to. I’m not comfortable with the word “fight,” but I’m not going to let that stop me from spreading awareness of the disease.
If you’re inclined to donate to the cause, the American Kidney Fund is doubling your donation this month. They also offer an advocacy program, as well as free screenings, activity days, financial assistance, and kidney education in addition to transplant and kidney donation information,
“Follow these healthy lifestyle tips to take charge of your kidney health.
Meet regularly with your health care team. Staying connected with your doctor, whether in-person or using telehealth via phone or computer, can help you maintain your kidney health.
Manage blood pressure and monitor blood glucose levels. Work with your health care team to develop a plan to meet your blood pressure goals and check your blood glucose level regularly if you have diabetes.
Take medicine as prescribed and avoid NSAIDs like ibuprofen and naproxen. Your pharmacist and doctor need to know about all the medicines you take.
Aim for a healthy weight. Create a healthy meal plan and consider working with your doctor to develop a weight-loss plan that works for you.
Reduce stress and make physical activity part of your routine. Consider healthy stress-reducing activities and get at least 30 minutes or more of physical activity each day.
Make time for sleep. Aim for 7 to 8 hours of sleep per night.
Quit smoking. If you smoke, take steps to quit.
It may seem difficult, but small changes can go a long way to keeping your kidneys and you healthier for longer.
As for me, I’ll continue to blog my brains out [just as I declared in last week’s blog] until more and more people are aware of the kidneys and kidney disease. Same goes for the Instagram, Facebook, Twitter, Pinterest, and LinkedIn accounts, and the SlowItDownCKDbook series. It’s all about kidney disease.
Ever since I had the surgery that removed part of my pancreas, my gall bladder, and my spleen while saving my life, I’ve had a superabundance of flatulence and belching. Remaining delighted that I’m alive, I’m still, well, embarrassed by this. I called the surgeon to see if this were normal. He hadn’t prescribed any long-term medication, so I think he was a bit surprised at my question. His answer was no.
Hmmm, maybe it was another medication since medication can be the source of both belching and flatulence. I called all my other doctors (and there were plenty). Nope, no one had prescribed a medication that would cause this. I’m fairly careful with my diet, so what could be the cause?
Ah, there I am starting in the middle again. Let’s go back to what each of these terms is.
“Flatulence is passing gas from the digestive system out of the back passage. [Gail here: I love how delicately that’s phrased.] It’s more commonly known as ‘passing wind,’ or ‘farting’.
Farting is often laughed about, but excessive flatulence can be embarrassing and make you feel uncomfortable around others. However, it can usually be controlled with changes to your diet and lifestyle.
Flatulence is a normal biological process and is something everyone experiences regularly. Some people pass wind only a few times a day, others a lot more, but the average is said to be about 5 to 15 times a day.”
While I like how easily I understood the definition, I wanted a little bit more and to find out about belching, too. Fortis Memorial Research Institute helped here and even threw in a bit about bloating – which seems to go along with belching and flatulence. It also explained what the pain you might experience with these three is:
“Belching is a normal process and results from swallowed air accumulating in the stomach. The [sic] can be subsequently passed as rectal gas (flatus) also.
Bloating is the subjective feeling that the abdomen is full but does not necessarily mean that the abdomen is enlarged.
Flatulence refers to the passage of rectal gas. The gas is generally a combination of swallowed air and gas produced by the action of colon bacteria on undigested food.
Gas accumulation can lead to pain which could seem like gallbladder pain or pain that can radiate up to the chest and seem like cardiac pain.”
This was more informative, but I still wanted to find out more about this subject. (I guess I’m just never satisfied!). The MayoClinic provided me with that:
“Flatulence: Gas buildup in the intestines
Gas in the small intestine or colon is typically caused by the digestion or fermentation of undigested food by bacteria found in the bowel. Gas can also form when your digestive system doesn’t completely break down certain components in foods, such as gluten, found in most grains, or the sugar in dairy products and fruit.
Other sources of intestinal gas may include:
Food residue in your colon
A change in the bacteria in the small intestine
Poor absorption of carbohydrates, which can upset the balance of helpful bacteria in your digestive system
Constipation, since the longer food waste remains in your colon, the more time it has to ferment
A digestive disorder, such as lactose or fructose intolerance or celiac disease”
There must be a way to cut down on belching and flatulence, I thought. Even if it’s normal, maybe it doesn’t have to happen so very often. So, I turned to my old buddy, Everyday Health to see if I could find some of the causative behaviors:
“Eating high-fiber foods like beans, legumes, fruits, vegetables, and whole grains
Drinking carbonated beverages
Chewing gum
Eating too quickly or talking while chewing, which results in swallowing more air
Drinking through a straw
Consuming artificial sweeteners
Chronic intestinal diseases like diverticulitis or inflammatory bowel disease
Food intolerances like celiac disease or lactose intolerance
Bacterial overgrowth in the small bowel”
That sounds easy enough. Yet, something was missing for me. I’d had cancer and still have chronic kidney disease. Is there some kind of connection? I found none with cancer, but Kidney Health Australia did make the connection between chronic kidney disease, and belching, bloating, and flatulence.
“Reduced kidney function can lead to bowel problems such as constipation and diarrhoea. This can cause stomach discomfort including pain, bloating, gas and nausea. A renal dietitian or renal nurse may be able to suggest how to safely increase the fibre in your diet. Gentle exercise such as walking can also help relieve discomfort. Medications can also provide relief.”
It’s the gas you produce that causes bloating (sometimes), belching, and flatulence. Remember that the Mayo Clinic cited constipation can contribute to these. Now we find that “reduced kidney function” can lead to constipation.
That’s what ckd is: a progression in the decline of your kidney function for at least three months.
Your flatulence, bloating, and/or belching may also be a complication of another problem. Check in with your medical team. You have to remember that I am not a doctor and have never claimed to be one.
Healthline suggests the following conditions may be the cause:
“If your diet doesn’t contain a large amount of carbohydrates or sugars, and you don’t swallow excessive air, your excessive flatulence may be due to a medical condition.
Potential conditions underlying flatulence range from temporary conditions to digestive problems. Some of these conditions include:
constipation
gastroenteritis
food intolerances, such as lactose intolerance
irritable bowel syndrome (IBS)
Crohn’s disease
celiac disease
diabetes
eating disorders
ulcerative colitis
dumping syndrome
gastroesophageal reflux disease (GERD)
autoimmune pancreatitis
peptic ulcers”
Uh-oh, did you notice “diabetes” in the list above? That’s the second most prevalent cause of CKD and vice-versa.
Hopefully, today’s blog has told you everything you always wanted to know about ckd & flatulence, belching, and bloating, but were afraid to ask (with apologies to Woody Allen).
Cute, huh? Especially since I’ll be writing about feces or, as it’s commonly called these days, poo. Defecation (or pooing, if you’d rather) is an important topic for those of us with Chronic Kidney Disease. Did you know CKD can lead to constipation?
“Constipation can be caused by a variety of medications. These medications affect the nerve and muscle activity in the large intestine (colon) and may also bind intestinal liquid. This may result in slowed colonic action (slow and/or difficult passing of stool).”
“Constipation happens because your colon absorbs too much water from waste (stool/poop), which dries out the stool making it hard in consistency and difficult to push out of the body.
To back up a bit, as food normally moves through the digestive tract, nutrients are absorbed. The partially digested food (waste) that remains moves from the small intestine to the large intestine, also called the colon. The colon absorbs water from this waste, which creates a solid matter called stool. If you have constipation, food may move too slowly through the digestive tract. This gives the colon more time – too much time – to absorb water from the waste. The stool becomes dry, hard, and difficult to push out.”
We’re Chronic Kidney Disease patients. That means some of the foods recommended to alleviate constipation may not be allowed on our renal diets. For instance, dried raisin, apricots, and prunes are too high in potassium for CKD patients, although they are helpful if you’re experiencing constipation. You need to speak with your renal dietitian before changing your diet.
I turned to a new site, BMC at https://rrtjournal.biomedcentral.com/articles/10.1186/s41100-019-0246-3 for information about constipation that is particular to CKD patients. BMC has “an evolving portfolio of some 300 peer-reviewed journals, sharing discoveries from research communities in science, technology, engineering and medicine,” as stated on their website.
“Accumulating evidence has revealed a relationship between constipation and cardiovascular disease and CKD. The pathogenesis of constipation in CKD patients is multifactorial: decreased physical activity, comorbidities affecting bowel movement, such as diabetes mellitus, cerebrovascular disease, and hyperparathyroidism, a restricted dietary intake of plant-based fiber-rich foods, and multiple medications, including phosphate binders and potassium-binding resins, have all been implicated. CKD is associated with alterations in the composition and function of the gut microbiota, so-called gut dysbiosis.”
“Gut microbiota dysbiosis, also known as intestinal or gastrointestinal dysbiosis, refers to a condition in which there is an imbalance of the microorganisms within our intestines. These microorganisms, collectively known as gut flora, consist predominantly of various strains of bacteria, and to a lesser extent include fungi and protozoa. The gut flora are essential for digestion and immune functioning…. A state of dysbiosis, therefore, will result in digestive and other systemic symptoms.”
Aha, so that’s why I take probiotics. I not only have CKD, but Diabetes Type 2, and have had chemotherapy which is known to cause this problem. I always wondered what the probiotics did for me. We’ll find out right now. WebMD at https://www.webmd.com/digestive-disorders/what-are-probiotics was helpful here:
“Researchers are trying to figure out exactly how probiotics work. Some of the ways they may keep you healthy:
When you lose ‘good’ bacteria in your body, for example after you take antibiotics, probiotics can help replace them.
They can help balance your ‘good’ and ‘bad’ bacteria to keep your body working the way it should.”
Prebiotics are also recommended. I get it that ‘pre’ is a suffix (group of letters added before a word to change its meaning) indicating ‘before,’ but still, what do they do for us? Here’s what the Mayo Clinic at https://www.mayoclinic.org/prebiotics-probiotics-and-your-health/art-20390058 has to say about prebiotics,
“Prebiotics are specialized plant fibers. They act like fertilizers that stimulate the growth of healthy bacteria in the gut.
Prebiotics are found in many fruits and vegetables, especially those that contain complex carbohydrates, such as fiber and resistant starch. These carbs aren’t digestible by your body, so they pass through the digestive system to become food for the bacteria and other microbes.”
To sum it all up:
“Constipation is one of the most common gastrointestinal disorders among patients with chronic kidney disease (CKD) partly because of their sedentary lifestyle, low fiber and fluid intake, concomitant medications (e.g., phosphate binders), and multiple comorbidities (e.g., diabetes). Although constipation is usually perceived as a benign, often self-limited condition, recent evidence has challenged this most common perception of constipation. The chronic symptoms of constipation negatively affect patients’ quality of life and impose a considerable social and economic burden. Furthermore, recent epidemiological studies have revealed that constipation is independently associated with adverse clinical outcomes, such as end-stage renal disease (ESRD), cardiovascular (CV) disease, and mortality, potentially mediated by the alteration of gut microbiota and the increased production of fecal metabolites. Given the importance of the gut in the disposal of uremic toxins and in acid-base and mineral homeostasis with declining kidney function, the presence of constipation in CKD may limit or even preclude these ancillary gastrointestinal roles, potentially contributing to excess morbidity and mortality….”
Thank you to the National Institutes of Health’s U.S. Library of Medicine’s National Center for Biotechnology Information at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7000799/ for their summary of the problem. Before I end this blog, I ask you to make sure you notice the mention of “the disposal of uremic toxins” above.
“1: a portion of a substance adhering together in a thick nondescript mass (as of clay or gum)
2 a: a roundish viscous lump formed by coagulation of a portion of liquid or by melting
b: a coagulated mass produced by clotting of blood”
You’re right – it’s the second definition we’ll be dealing with today. Why? A long-time reader was telling me about his blood clot when I suddenly realized I had no idea if there were any connection at all between Chronic Kidney Disease and blood clots.
“CKD may put you at higher risk for VTE. The reasons for this are not well understood. The connection may depend on what caused your CKD and how much kidney damage you have. No matter the reason, CKD may make it easier for your body to form blood clots. The risk for VTE is seen more often in people with nephrotic syndrome (a kidney problem that causes swelling, usually of the ankles, a high level of protein in the urine, and a low level of a protein called albumin in the blood).”
“Venous thromboembolism (VTE) is a condition in which a blood clot forms most often in the deep veins of the leg, groin or arm (known as deep vein thrombosis, DVT) and travels in the circulation, lodging in the lungs (known as pulmonary embolism, PE).”
How could I have CKD for over a dozen years and not know this? Many thanks to my reader and online friend for bringing it up.
“Duplex ultrasonography is an imaging test that uses sound waves to look at the flow of blood in the veins. It can detect blockages or blood clots in the deep veins. It is the standard imaging test to diagnose DVT. A D-dimer blood test measures a substance in the blood that is released when a clot breaks up.”
Let’s take a closer look at the D-dimer blood test. That’s another new one for me. My old standby, MedlinePlus (This time at https://medlineplus.gov/lab-tests/d-dimer-test/.) offered the following which more than satisfactorily answered my question.
“A D-dimer test looks for D-dimer in blood. D-dimer is a protein fragment (small piece) that’s made when a blood clot dissolves in your body.
Blood clotting is an important process that prevents you from losing too much blood when you are injured. Normally, your body will dissolve the clot once your injury has healed. With a blood clotting disorder, clots can form when you don’t have an obvious injury or don’t dissolve when they should. These conditions can be very serious and even life-threatening. A D-dimer test can show if you have one of these conditions.”
By the way, MedlinePlus is part of the U.S. National Library of Medicine which, in turn, is part of the National Institutes of Health.
This brings me to another question. How would you or your doctor even know you may need this test?
“According to the Centers for Disease Control and Prevention (CDC), about half of people with DVT don’t have symptoms. Any symptoms that do occur will be in the affected leg or the area where the clot is found. Symptoms can include:
pain
redness of the skin
warmth of the skin
swelling of the area
If the clot moves into the lungs and you develop PE, you may have symptoms such as:
chest pain, which may get worse when you breathe deeply or cough
Now we know what VTE is, what symptoms you may experience, and the test to take to confirm that you do, indeed, have VTE. You know what comes next. How do we treat VTE once it’s confirmed?
“Blood thinners. These drugs don’t break up the clot, but they can stop it from getting bigger so your body has time to break it down on its own. They include heparin, low-molecular-weight heparin, apixaban (Eliquis), edoxaban (Savaysa), rivaroxaban (Xarelto), and warfarin (Coumadin).
Clot-busting drugs. These medicines are injections that can break up your clot. They include drugs like tPA (tissue plasminogen activator).
Surgery. In some cases, your doctor may need to put a special filter into a vein, which can stop any future clots from getting to your lungs. Sometimes, people need surgery to remove a clot.
Even after you recover from a VTE and you’re out of the hospital, you’ll probably still need treatment with blood thinners for at least 3 months. That’s because your chances of having another VTE will be higher for a while.”
“Ask your doctor about need for ‘blood thinners’ or compression stockings to prevent clots, whenever you go to the hospital
Lose weight, if you are overweight
Stay active
Exercise regularly; walking is fine
Avoid long periods of staying still
Get up and move around at least every hour whenever you travel on a plane, train, or bus, particularly if the trip is longer than 4 hours
Do heel toe exercises or circle your feet if you cannot move around
Stop at least every two hours when you drive, and get out and move around
Drink a lot of water and wear loose fitted clothing when you travel
Talk to your doctor about your risk of clotting whenever you take hormones, whether for birth control or replacement therapy, or during and right after any pregnancy
Follow any self-care measures to keep heart failure, diabetes, or any other health issues as stable as possible”
And we have yet another reason to be extra cautious if you have CKD.
It’s true, and it’s not only me. It’s you, too, if you have Chronic Kidney Disease. ‘What do I mean?’ you ask. It’s your immune system that’s been compromised by your CKD. ‘HOW?’ you demand. That’s what today’s blog is going to explain.
Let’s start the usual way: at the beginning. So, what’s this immune system I mentioned? I turned to Medline Plus, a part of the U.S. National Library of Medicine which, in turn, is a division of the National Institutes of Health at https://medlineplus.gov/immunesystemanddisorders.html
“Your immune system is a complex network of cells, tissues, and organs that work together to defend against germs. It helps your body to recognize these ‘foreign’ invaders. Then its job is to keep them out, or if it can’t, to find and destroy them.”
“…Having kidney disease and kidney failure can weaken your immune system, making it easier for infections to take hold. In fact, doctors and researchers have found that most infections, …, are worse in people with kidney disease. People with a kidney transplant also have weakened immune systems. This is because antirejection medicines (‘immunosuppressants’), which protect the body from rejecting the transplanted kidney, suppress the immune system.”
That makes sense. But exactly how does CKD compromise this system?
According to a British Society for Immunology study published in PubMed [“PubMed Central (PMC) is a free archive of biomedical and life sciences journal literature at the U.S. National Institutes of Health’s National Library of Medicine (NIH/NLM),” as stated on their website. NCBI is The National Center for Biotechnology Information.] at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5904695/:
“The immune system and the kidneys are closely linked. In health the kidneys contribute to immune homeostasis, while components of the immune system mediate many acute forms of renal disease and play a central role in progression of chronic kidney disease. A dysregulated immune system can have either direct or indirect renal effects. Direct immune‐mediated kidney diseases are usually a consequence of autoantibodies directed against a constituent renal antigen, …. Indirect immune‐mediated renal disease often follows systemic autoimmunity with immune complex formation, but can also be due to uncontrolled activation of the complement pathways. Although the range of mechanisms of immune dysregulation leading to renal disease is broad, the pathways leading to injury are similar. Loss of immune homeostasis in renal disease results in perpetual immune cell recruitment and worsening damage to the kidney. Uncoordinated attempts at tissue repair, after immune‐mediated disease or non‐immune mediated injury, result in fibrosis of structures important for renal function, leading eventually to kidney failure.”
Hmmm, it seems my linking function is not working for this URL. No loss, just copy and paste the URL if you’d like to read more about the immune system and the kidneys.
There are a few medical terms in the above paragraph that you may need defined. Thank you, my all-time favorite dictionary, the Merriam-Webster, for helping us out here.
Antibody: any of a large number of proteins of high molecular weight that are produced normally by specialized B cells after stimulation by an antigen and act specifically against the antigen in an immune response, that are produced abnormally by some cancer cells, and that typically consist of four subunits including two heavy chains and two light chains
Antigen: any substance (such as an immunogen or a hapten [Gail here: Bing defines this as “a small molecule which, when combined with a larger carrier such as a protein, can elicit the production of antibodies which bind specifically to it (in the free or combined state.]) foreign to the body that evokes an immune response either alone or after forming a complex with a larger molecule (such as a protein) and that is capable of binding with a product (such as an antibody or T cell) of the immune response
Eat colorful fruits and vegetables. (Within your kidney diet, of course.)
Consider herbs and supplements. (Check with your nephrologist first.)
Exercise.
Sleep an adequate number of hours.
Cut back on alcohol consumption.
Stop smoking.
Keep washing those hands.
Some doctors, such as Dr. Suzanne Cassel, an immunologist at Cedars-Sinai, think we need to balance our immune systems rather than strengthen them. ” ‘You actually don’t want your immune system to be stronger, you want it to be balanced,’ Dr. Cassel says. ‘Too much of an immune response is just as bad as too little response.’
Dr. Cassel says most of the things people take to boost their immune system, such as vitamins or supplements, don’t have any effect on your immune response.”
Obviously, all doctors don’t agree. Whether you want to balance your immune system or strengthen it, the suggestions above will be helpful. Notice whether or not we’re in the middle of a pandemic, washing your hands frequently can help your immune system. Most of the suggestions from WebMD may be surprising to you since they are lifestyle changes and/or are the same ones suggested in general for CKD patients. There’s got to be something to them if they can both help with your CKD and your immune system. Why not try the suggestions you’re not already adhering to?
By the way, to the reader who asked why chocolate is not good for CKD patients, it’s loaded with potassium. In addition, many CKD patients also have diabetes. The sugar content in chocolate is not going to do them any good.
This is one of those topics we don’t like to talk about, but have probably each experienced at one time or another. There are other causes of constipation, but today, we’ll stick with that caused by drugs. Mind you, we’re not talking about party drugs. Rather, it’s the drugs that are prescribed for you that may cause constipation which I’m writing about.
“Constipation can be caused by a variety of medications. These medications affect the nerve and muscle activity in the large intestine (colon) and may also bind intestinal liquid. This may result in slowed colonic action (slow and/or difficult passing of stool).”
“The etiology [Gail here. That means the cause of the disease.] of constipation is usually multifactorial, but it can be broadly divided into two main groups …: primary constipation and secondary constipation.
Primary constipation
Primary (idiopathic, functional) constipation can generally be subdivided into the following three types:
NTC is the most common subtype of primary constipation. Although the stool passes through the colon at a normal rate, patients find it difficult to evacuate their bowels. Patients in this category sometimes meet the criteria for IBS with constipation (IBS-C). The primary difference between chronic constipation and IBS-C is the prominence of abdominal pain or discomfort in IBS. Patients with NTC usually have a normal physical examination.
STC is characterized by infrequent bowel movements, decreased urgency, or straining to defecate. It occurs more commonly in female patients. Patients with STC have impaired phasic colonic motor activity. They may demonstrate mild abdominal distention or palpable stool in the sigmoid colon.
Pelvic floor dysfunction is characterized by dysfunction of the pelvic floor or anal sphincter. Patients often report prolonged or excessive straining, a feeling of incomplete evacuation, or the use of perineal or vaginal pressure during defecation to allow the passage of stool, or they may report digital evacuation of stool.”
We won’t be dealing with secondary constipation today since that doesn’t include drugs in its etiology.
“Constipation happens because your colon absorbs too much water from waste (stool/poop), which dries out the stool making it hard in consistency and difficult to push out of the body.
To back up a bit, as food normally moves through the digestive tract, nutrients are absorbed. The partially digested food (waste) that remains moves from the small intestine to the large intestine, also called the colon. The colon absorbs water from this waste, which creates a solid matter called stool. If you have constipation, food may move too slowly through the digestive tract. This gives the colon more time – too much time – to absorb water from the waste. The stool becomes dry, hard, and difficult to push out.”
Imagine, drugs to improve your health taxing your health. Luckily, since you need to take the prescribed drugs to alleviate whatever your medical diagnosis is, there are methods to relieve your constipation. Here’s WebMD’s (https://www.webmd.com/digestive-disorders/constipation-relief-tips) advice:
“One way to keep things moving is by getting enough fiber in your diet, which makes stool bulkier and softer so it’s easier to pass. Gradually increase the amount of fiber in your diet until you’re getting at least 20 to 35 grams of fiber daily.
Good fiber sources include:
Bran and other whole grains found in cereals, breads, and brown rice
Vegetables such as Brussels sprouts, carrots, and asparagus
Fresh fruits, or dried fruits such as raisins, apricots, and prunes”
Beans
While you’re having an issue with constipation, limit foods that are high in fat and low in fiber, like cheese and other dairy products, processed foods, and meat. They can make constipation worse.
And on the subject of diet, water is important for preventing constipation, too. Try to drink at least 8 glasses of water a day.
Also, exercise regularly. Moving your body will keep your bowels moving, too.”
Wait a minute. We’re Chronic Kidney Disease patients. That’s means some of the foods listed above may not be allowed on our renal diets. For instance, dried raisin, apricots, and prunes are too high in potassium for CKD patients. You need to speak with your renal dietitian before changing your diet.
As Benjamin Franklin stated, “an ounce of prevention is worth a pound of cure.” Let’s see what we can find on prevention.
“Increasing your fiber intake: Fiber-rich foods, such as fruits, vegetables and whole grains, all help improve gut function. If you have bowel sensitivity, you’ll want to avoid high-fructose fruits, such as apples, pears and watermelon, which can cause gas.
Getting more exercise: Regular exercise can help keep stool moving through the colon.
Drinking more water: Aim for eight glasses daily, and avoid caffeine, as it can be dehydrating.
Go when you feel like it: When you feel the urge to go, don’t wait.”
I’ve already mentioned that I read a lot while undergoing chemotherapy for my pancreatic cancer. I don’t have the energy for much else, although I do find my energy slowly increasing day by day. Often, I come across words or terms that are new to me as I read. One such term is ‘hypertensive nephrosclerosis.’ That’s a mouthful, so let’s start slowly.
‘Hypertensive’ is not a problem since we know that hyper means,
“hyper– a prefix appearing in loanwords from Greek, where it meant “over,” usually implying excess or exaggeration (hyperbole); on this model used, especially as opposed to hypo-, in the formation of compound words (hyperthyroid).”
Thank you, Dictionary.com at https://www.dictionary.com/browse/hyper-. A little reminder: a prefix is a group of letters added at the beginning of a word which changes its meaning. Aren’t you glad I was an English teacher for over forty years?
You’ve probably already figured out that ‘tensive’ has to do with some kind of tension. According to Dictionary.com again, but this time at https://www.dictionary.com/browse/tensive?s=ts, it means,
“adjective
stretching or straining”
That is a sort of tension, so you’re right. Add the prefix to the root word and suffix and you get ‘hypertension.’ Maybe a little grammar lesson would help here. A suffix is a group of letters added at the end of a word that change its meaning by expressing tendency, disposition, function, connection, etc. (By the way, some of this was taken from – yep – Dictionary.com again. This time at https://www.dictionary.com/browse/-ive?s=t.) What else? Oh, yes, ‘root.’ That’s the main part of the word; in this word, it’s tens. I know, I know, you didn’t come here for a grammar lesson.
Good thing ‘nephrosclerosis’ is a compound word. We know all about ‘nephro’ since it means kidney. And ‘sclerosis?’ That means hardening. This is a good point to mention this can be fatal. A former colleague recently died of sclerosis.
Nephrosclerosis: A progressive disease of the kidneys that results from sclerosis (hardening) of the small blood vessels in the kidneys. Nephrosclerosis is most commonly associated with hypertension or diabetes and can lead to kidney failure.
“The term hypertensive nephrosclerosis has traditionally been used to describe a clinical syndrome characterized by long-term essential hypertension, hypertensive retinopathy, left ventricular hypertrophy, minimal proteinuria, and progressive renal insufficiency. Most cases are diagnosed based solely on clinical findings….”
Okay, let’s break down the definition of what we just added together to understand this term. You already know what ‘hypertension’ and ‘proteinuria’ are from reading my blogs. If you forgot, use the click throughs in the above definition. That leaves ‘hypertensive retinopathy’ and ‘left ventricular hypertrophy’ since we also know what ‘progressive renal insufficiency’ is.
‘Hypertensive retinopathy’ is summarized by DoveMed, a new site for me whose stated mission is
“We provide reliable unbiased medical information to healthcare consumers and providers by leveraging our unique ecosystem of world class products and services.”
“Hypertensive Retinopathy (HR) refers to abnormal changes of the retina that is located in the back of the eye, due to chronic hypertension (high blood pressure)
The retinal arteries are autoregulated, meaning they can control their own shape based on changes in systemic blood pressure. However, at extremely high blood pressures, such as a blood pressure of 140/110 mmHg or over, they are unable to autoregulate. This can result in retinal complications
Depending on the severity of the signs and symptoms, Hypertensive Retinopathy can be classified to 4 stages – stage 1, 2, 3, and 4. Stage 1 Hypertensive Retinopathy has mild signs and symptoms, whereas Stage 4 Hypertensive Retinopathy has severe signs and symptoms
These changes typically occur in individuals who have had very high blood pressure for several years. The signs and symptoms of Hypertensive Retinopathy may include leakage of fats from the blood vessels, retinal edema (fluid in the retina), and swelling of the optic nerves
Some of the complications can include lack of oxygen delivered to the retina, as well as swelling of the macula and optic nerve that can result in the vision being affected
The treatment typically consists of controlling systemic hypertension with medications. Prognosis is generally good for individuals with stage 1 or 2 Hypertensive Retinopathy”
“Left ventricular hypertrophy is enlargement and thickening (hypertrophy) of the walls of your heart’s main pumping chamber (left ventricle).
Left ventricular hypertrophy can develop in response to some factor — such as high blood pressure or a heart condition — that causes the left ventricle to work harder. As the workload increases, the muscle tissue in the chamber wall thickens, and sometimes the size of the chamber itself also increases. The enlarged heart muscle loses elasticity and eventually may fail to pump with as much force as needed.
Left ventricular hypertrophy is more common in people who have uncontrolled high blood pressure. But no matter what your blood pressure is, developing left ventricular hypertrophy puts you at higher risk of a heart attack and stroke.
Treating high blood pressure can help ease your symptoms and may reverse left ventricular hypertrophy.”
Adding all this information together, it’s clear that hypertensive blood pressure is going to do you no good in any way. So what do we do to avoid high blood pressure? That’s right! And the CDC backs you up. Take a look at https://www.cdc.gov/bloodpressure/prevent.htm.
“Prevent High Blood Pressure
….Eat a Healthy Diet
Choose healthy meal and snack options to help you avoid high blood pressure and its complications. Be sure to eat plenty of fresh fruits and vegetables.
Talk with your health care team about eating a variety of foods rich in potassium, fiber, and protein and lower in salt (sodium) and saturated fat. For many people, making these healthy changes can help keep blood pressure low and protect against heart disease and stroke.
The DASH (Dietary Approaches to Stop Hypertension) eating plan is a healthy diet plan with a proven record of helping people lower their blood pressure….
Having overweight or obesity increases your risk for high blood pressure. To determine whether your weight is in a healthy range, doctors often calculate your body mass index (BMI). If you know your weight and height, you can calculate your BMI at CDC’s Assessing Your Weight website. Doctors sometimes also use waist and hip measurements to assess body fat.
Talk with your health care team about ways to reach a healthy weight, including choosing healthy foods and getting regular physical activity.
Be Physically Active
Physical activity can help keep you at a healthy weight and lower your blood pressure. The Physical Activity Guidelines for Americans recommends that adults get at least 2 hours and 30 minutes of moderate-intensity exercise, such as brisk walking or bicycling, every week. That’s about 30 minutes a day, 5 days a week. Children and adolescents should get 1 hour of physical activity every day.
Smoking raises your blood pressure and puts you at higher risk for heart attack and stroke. If you do not smoke, do not start. If you do smoke, quitting will lower your risk for heart disease. Your doctor can suggest ways to help you quit.
Do not drink too much alcohol, which can raise your blood pressure. Men should have no more than 2 alcoholic drinks per day, and women should have no more than 1 alcoholic drink per day. Visit the CDC’s Alcohol and Public Health website for more information.
Welcome to the next to last day of National Kidney Month, 2020. Of course, that doesn’t mean you should stop taking care of your kidneys or spreading Chronic Kidney Disease awareness once National Kidney Month is over, but I don’t have to tell you that, do I? What I’d like to tell you about instead is the ins and outs of National Kidney Month.
In my latest book (Cancer has definitely slowed the arrival of SlowItDownCKD 2019, but soon, my friends, soon.) SlowItDownCKD 2018, I wrote:
“As usual, let’s start at the beginning. What is National Kidney Month? Personalized Cause at https://www.personalizedcause.com/health-awareness-cause-calendar/national-kidney-month has a succinct explanation for us. By the way, while I’m not endorsing them since the site is new to me, I should let you know they sell the green ribbons for National Kidney Month that you’ll probably be seeing hither and yon all month. [Added today: Come to think of it, some readers have asked me where to get CKD ribbons. This is what this site sells among other things.]
‘National Kidney Month, observed in March and sponsored by the National Kidney Foundation, is a time to increase awareness of kidney disease, promote the need for a cure, and spur advocacy on behalf of those suffeing [sic] with the emotional, financial and physical burden of kidney disease. The National Kidney Foundation is the leading organization in the U.S. dedicated to the awareness, prevention and treatment of kidney disease for hundreds of thousands of healthcare professionals, millions of patients and their families, and tens of millions of Americans at risk.’
‘Focus on the Kidneys During National Kidney Month in March
March is National Kidney Month and the NKF is urging all Americans to give their kidneys a second thought and a well-deserved checkup. Kidneys filter 200 liters of blood a day, help regulate blood pressure and direct red blood cell production. But they are also prone to disease; 1 in 3 Americans is at risk for kidney disease due to diabetes, high blood pressure [Added today: This year’s theme for National Kidney Month is high blood pressure and your kidneys.] or a family history of kidney failure. There are more than 30 million Americans [Added today: 31 million this year] who already have kidney disease, and most don’t know it because there are often no symptoms until the disease has progressed….’
I wanted to share this quote from the American Kidney Fund with you, both as a CKD awareness advocate and a woman:
‘Kidney disease is a silent killer that disproportionately affects women who are often the primary caregivers for loved ones with the disease, are more likely to become living donors but less likely to receive a transplant, and are at higher risk for CKD,’ said LaVarne A. Burton, president and chief executive officer of AKF. ‘Because women with kidney disease may also face other health issues, including infertility, pregnancy complications, bone disease and depression, AKF is using Kidney Month to let women know we are here to support them and to provide resources that will answer their questions and concerns.’
The Renal Support Network at https://www.rsnhope.org/ is working even more emphatically to spread kidney disease awareness this month, too:
‘March is National Kidney Month. This is a special time set aside to raise awareness about kidney health and activities. RSN invites members of the kidney community, our friends and our families to join in the conversation.’
This on top of their usual. For those that are not familiar with this group, the following statement is from their website.
‘Since 1993 RSN has created and continues to produce a vast collection of information about kidney disease. Feel free to share our National Kidney Month page, a favorite story, KidneyTalk™ show or awareness image on social media using the hashtag #KidneyMonth and be sure to tag us @RSNhope.’
DaVita Kidney Care at https://www.davita.com/education/resources offers many resources (as the website’s URL assures us) to help understand both CKD and dialysis. Some of their offerings are:
“March is National Kidney Month, a time when communities across the country raise awareness about kidney disease. In partnership with the National Heart, Lung, and Blood Institute (NHLBI), this year’s focus is the link between high blood pressure and kidney disease.
If you have high blood pressure, you’re at risk for chronic kidney disease, a serious condition that can lead to stroke, heart attack, kidney failure, and death.
The good news is that you can help protect your kidneys by managing high blood pressure with these 6 healthy lifestyle habits.
Take medications as prescribed. Your doctor may prescribe blood pressure-lowering medications that are effective in slowing the development of kidney disease.
Aim for a healthy weight. If you are overweight or obese, losing even a small amount of weight can improve blood pressure readings.
Select healthier food and beverage options. Focus on fruits and vegetables, lean meat, whole grains, and other heart-healthy foods.
Try to quit smoking. If you smoke, take steps to quit.
Get enough sleep. Aim for 7 to 8 hours of sleep per night.
Manage stress and make physical activity part of your routine. Consider healthy stress-reducing activities and get at least 30 minutes or more of physical activity each day.
Learn more about high blood pressure and kidney disease
As for me, I’ll blog my brains out until more and more people are aware of kidney disease. Same goes for the Instagram, Facebook, Twitter, Pinterest, and LinkedIn accounts. It’s all about kidney disease awareness.
A few weeks ago, I received an email from Joe Russell. He works on health care policy issues for my Arizona Senator Sinema in Washington D.C., along with his colleague Sylvia Lee, policy advisor. He was letting me know both Sylvia and he would be in Arizona the following week, and holding a roundtable discussion with patients suffering from kidney disease, along with their providers, caregivers, and family members. They wanted to discuss a series of legislative proposals their office would be working on in the coming months, as well as gain a better understanding of the unique challenges patients with kidney disease face in Arizona. The National Kidney Foundation of Arizona recommended they reach out to me, given my work and experience on this topic.
Are you kidding, I thought. I’ve been trying to get someone in Arizona interested in the growth of CKD locally… and, of course, everywhere else, for over 12 years. Now, mind you, by 3:30 I’m exhausted (Damn chemo!), but I vowed to go even though it was later in the day (3 p.m.). And I did.
When I arrived, who did I see sitting at Senator Sinema’s table, but Raymond and Analyn Scott. They are the compilers of The 1 in 9 Tribe to which I had contributed a chapter. There were people from the National Kidney Foundation of Arizona, a transplant patient, my very own nephrologist (who is also Raymond’s) and Senator Sinema’s delegation.
Oh boy, I remember thinking, this is going to be good. And it was. Each person spoke to their own stage of CKD with Dr. DeSai (Raymond’s and my nephrologist) and the National Kidney Foundation of Arizona people speaking about all stages of CKD. I kept steering the discussion back to early stage treatment and awareness for all. It seemed all were in agreement with my ideas or, at least, they were interested.
But I want to let you know why I feel early intervention and general awareness are so important. This is a note I received from a reader.
”Please help. I just got blood results back from my yearly physical and saw that my eGFR was 55 and my creatinine was 1.09. After speaking to my GP she told me my results were nothing to ‘be concerned about’. Since the 2 above mentioned results were highlighted in red I figured perhaps I should ‘concern’ myself about it and research what it could possibly mean. I was shocked to read that it indicated kidney disease. When I told my doctor of my findings, she again pushed it off as nothing to worry about. Am I over reacting? Thanks for any help you can give me.”
Now we don’t know this reader’s age. That’s important because you lose one point off your Glomerular Filtration Rate every year once you hit the age of 40. For example, I turned 73 yesterday (Yes, it was a fun birthday with my family and friends despite the effects of chemo.). Subtract 40 from that and I have lost 33 points off my GFR simply by being alive and growing older. Considering the highest GFR is 120, although we usually use 100 for ease of figuring, my perfect GFR would be 87. But it’s not. It’s 55, so we know I have CKD, stage 3A just like this reader.
Nuts! I’m going on and on as if everyone reading this knew both what GFR is and the stages of CKD. Well, we’ll just correct that right now. According to MedlinePlus, part of the U.S. National Library of Medicine which, in turn, is part of the National Institutes of Health, at https://medlineplus.gov/ency/article/007305.htm.
“Glomerular filtration rate
Glomerular filtration rate (GFR) is a test used to check how well the kidneys are working. Specifically, it estimates how much blood passes through the glomeruli each minute. Glomeruli are the tiny filters in the kidneys that filter waste from the blood.
The blood sample is sent to a lab. There, the creatinine level in the blood sample is tested. Creatinine is a chemical waste product of creatine. Creatine is a chemical the body makes to supply energy, mainly to muscles.
The lab specialist combines your creatinine level with several other factors to estimate your GFR. Different formulas are used for adults and children. The formula includes some or all of the following:
“This is due to higher average muscle mass and creatinine generation rate in African Americans.”
So, why then, is it important to know if you’re only in stage 2 of CKD? Let me put it this way:
When I was first diagnosed with CKD, I was at a GFR of 39. That’s pretty low. Had I been tested earlier, I would have had more time to preserve more of my kidney function. While I’m now at about 55 GFR (just like my reader), it took years and years of hard work as far as diet, exercise, rest, sleep, avoiding anxiety, not drinking or smoking and making sure I paid special attention to my labs.
Imagine if I had known earlier that I had CKD. I could have started protecting my kidneys earlier, which may have meant I could avoid dialysis for longer… or maybe at all. It may have meant I wouldn’t reach the place where I needed a transplant, if I ever needed one.
If you are routinely checked via a blood test and urine test each time you see your family doctor – just like your heart and lungs are checked – you may be able to avoid being told you were in need of dialysis seemingly out of the blue. But you wouldn’t know to ask for these tests unless everyone is made aware of CKD and just how prevalent it is. Think about it.
We all know diabetes raises your risk of developing Chronic Kidney Disease. But why? What’s the mechanism behind the fact? As far as I’m concerned, it’s time to find out.
Let’s start with diabetes. The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health (NIH), which in turn is part of The U.S. Department of Health and Human Services at https://www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes offers this explanation.
“Diabetes is a disease that occurs when your blood glucose, also called blood sugar, is too high. Blood glucose is your main source of energy and comes from the food you eat. Insulin, a hormone made by the pancreas, helps glucose from food get into your cells to be used for energy. Sometimes your body doesn’t make enough—or any—insulin or doesn’t use insulin well. Glucose then stays in your blood and doesn’t reach your cells.
Over time, having too much glucose in your blood can cause health problems. Although diabetes has no cure, you can take steps to manage your diabetes and stay healthy.
Sometimes people call diabetes ‘a touch of sugar’ or ‘borderline diabetes.’”
Having just had a tumor removed from my pancreas, I’m well aware that it produces insulin as well as digestive enzymes. Without a pancreas to produce insulin, you would need insulin injections several times a day.
I got what diabetes is, but how it causes CKD was still not clear.
“When our bodies digest the protein we eat, the process creates waste products. In the kidneys, millions of tiny blood vessels (capillaries) with even tinier holes in them act as filters. As blood flows through the blood vessels, small molecules such as waste products squeeze through the holes. These waste products become part of the urine. Useful substances, such as protein and red blood cells, are too big to pass through the holes in the filter and stay in the blood.
Diabetes can damage this system. High levels of blood sugar make the kidneys filter too much blood. All this extra work is hard on the filters. After many years, they start to leak and useful protein is lost in the urine. Having small amounts of protein in the urine is called microalbuminuria.
When kidney disease is diagnosed early, during microalbuminuria, several treatments may keep kidney disease from getting worse. Having larger amounts of protein in the urine is called macroalbuminuria. When kidney disease is caught later during macroalbuminuria, end-stage renal disease, or ESRD, usually follows.
In time, the stress of overwork causes the kidneys to lose their filtering ability. Waste products then start to build up in the blood. Finally, the kidneys fail. This failure, ESRD, is very serious. A person with ESRD needs to have a kidney transplant or to have the blood filtered by machine (dialysis).”
Hmmm, now that we know what diabetes is and how it can cause CKD, maybe we need to look at ways to attempt to avoid diabetes.
“Losing weight and keeping it off.Weight control is an important part of diabetes prevention. You may be able to prevent or delay diabetes by losing 5 to 10 percent of your current weight. For example, if you weigh 200 pounds, your goal would be to lose between 10 to 20 pounds. And once you lose the weight, it is important that you don’t gain it back.
Following a healthy eating plan. It is important to reduce the amount of calories you eat and drink each day, so you can lose weight and keep it off. To do that, your diet should include smaller portions and less fat and sugar. You should also eat a variety of foods from each food group, including plenty of whole grains, fruits, and vegetables. It’s also a good idea to limit red meat, and avoid processed meats.
Get regular exercise. Exercise has many health benefits, including helping you to lose weight and lower your blood sugar levels. These both lower your risk of type 2 diabetes. Try to get at least 30 minutes of physical activity 5 days a week. If you have not been active, talk with your health care professional to figure out which types of exercise are best for you. You can start slowly and work up to your goal.
Don’t smoke. Smoking can contribute to insulin resistance, which can lead to type 2 diabetes. If you already smoke, try to quit.
Talk to your health care provider to see whether there is anything else you can do to delay or to prevent type 2 diabetes. If you are at high risk, your provider may suggest that you take one of a few types of diabetes medicines.”
This is a list from NIH: National Institute of Diabetes and Digestive and Kidney Diseases posted on MedLinePlus at https://medlineplus.gov/howtopreventdiabetes.html. Notice it’s mentioned that this is for type 2 diabetes.
“Type 1 diabetes is an autoimmune condition. It’s caused by the body attacking its own pancreas with antibodies. In people with type 1 diabetes, the damaged pancreas doesn’t make insulin…. With Type 2 diabetes, the pancreas usually produces some insulin. But either the amount produced is not enough for the body’s needs, or the body’s cells are resistant to it. Insulin resistance, or lack of sensitivity to insulin, happens primarily in fat, liver, and muscle cells.”
I’ve been reading a lot about dapagliflozin lately. That’s a word I didn’t know. And this is the perfect opportunity to learn about it. Ready? Let’s start.
The obvious first stop to my way of thinking was Medline Plus, part of the U.S. Library of Medicine, which in turn, is part of the Institutes of National Health at https://medlineplus.gov/druginfo/meds/a614015.html.
“Dapagliflozin is used along with diet and exercise, and sometimes with other medications, to lower blood sugar levels in patients with type 2 diabetes (condition in which blood sugar is too high because the body does not produce or use insulin normally). Dapagliflozin is in a class of medications called sodium-glucose co-transporter 2 (SGLT2) inhibitors. It lowers blood sugar by causing the kidneys to get rid of more glucose in the urine. Dapagliflozin is not used to treat type 1 diabetes (condition in which the body does not produce insulin and, therefore, cannot control the amount of sugar in the blood) or diabetic ketoacidosis (a serious condition that may develop if high blood sugar is not treated).
Over time, people who have diabetes and high blood sugar can develop serious or life-threatening complications, including heart disease, stroke, kidney problems, nerve damage, and eye problems. Taking dapagliflozin, making lifestyle changes (e.g., diet, exercise, quitting smoking), and regularly checking your blood sugar may help to manage your diabetes and improve your health. This therapy may also decrease your chances of having a heart attack, stroke, or other diabetes-related complications such as kidney failure, nerve damage (numb, cold legs or feet; decreased sexual ability in men and women), eye problems, including changes or loss of vision, or gum disease. Your doctor and other healthcare providers will talk to you about the best way to manage your diabetes.”
“SGLT2 inhibitors are a class of prescription medicines that are FDA-approved for use with diet and exercise to lower blood sugar in adults with type 2 diabetes. Medicines in the SGLT2 inhibitor class include canagliflozin, dapagliflozin, and empagliflozin. They are available as single-ingredient products and also in combination with other diabetes medicines such as metformin. SGLT2 inhibitors lower blood sugar by causing the kidneys to remove sugar from the body through the urine. The safety and efficacy of SGLT2 inhibitors have not been established in patients with type 1 diabetes, and FDA has not approved them for use in these patients.”
There are also quite a few warnings about amputations and urinary tract infections caused by SGLT2 inhibitors on this site, although they are dated 8/20/18.
Wait a minute. According to their chart, dapagliflozin is not recommended if your GFR is below 60, or stage 3 CKD. Canagliflozin is not recommended if your GFR is below 45. Your kidney function is a big factor in whether or not this drug can be prescribed for you.
But why? Exactly how do the kidneys process this drug? The following diagram from The National Center for Biotechnology Information, part of the U.S. National Library, which in turn (again) is part of the National Institutes of Health at https://www.ncbi.nlm.nih.gov/core/lw/2.0/html/tileshop_pmc/tileshop_pmc_inline.html?title=Click%20on%20image%20to%20zoom&p=PMC3&id=3889318_13300_2013_42_Fig1_HTML.jpg will give you the visual. Basically, the SLGT2 inhibitor prevents the glucose in your blood from re-entering your blood stream after your blood has been filtered. The glucose has nowhere to go, so it exits your body via your urine along with the other wastes.
”On Aug. 29, 2018, the FDA issued a warning that cases of a rare but serious infection of the genitals and area around the genitals have been reported with the class of type 2 diabetes medicines called SGLT2 inhibitors. This serious rare infection, called necrotizing fasciitis of the perineum, is also referred to as Fournier’s gangrene.
SGLT2 inhibitors are FDA-approved for use with diet and exercise to lower blood sugar in adults with type 2 diabetes. SGLT2 inhibitors lower blood sugar by causing the kidneys to remove sugar from the body through the urine. First approved in 2013, medicines in the SGLT2 inhibitor class include canagliflozin, dapagliflozin, empagliflozin, and ertugliflozin. In addition, empagliflozin is approved to lower the risk of death from heart attack and stroke in adults with type 2 diabetes and heart disease. Untreated, type 2 diabetes can lead to serious problems, including blindness, nerve and kidney damage, and heart disease.
Seek medical attention immediately if you experience any symptoms of tenderness, redness, or swelling of the genitals or the area from the genitals back to the rectum, and have a fever above 100.4 F or a general feeling of being unwell. These symptoms can worsen quickly, so it is important to seek treatment right away.
On May 15, 2015, the FDA informed the public that SGLT2 inhibitors have been associated with increased risk of ketoacidosis in people with diabetes.
Common side effects
The most common side effect of SGLT2 inhibitors include:
Whoa. It looks like there will have to be some serious discussions with your nephrologist before you agree to taking a SLGT2 inhibitor should he or she suggest it. Make sure you have your list of questions ready and someone to listen carefully and take notes.
What! As if staying in the hospital for six to thirteen days weren’t enough, it turned out that I would be in a rehabilitation center for an additional six to eight weeks. Again, while this was for pancreatic cancer, many Chronic Kidney Disease patients who have had surgery may require a stay in such places, too. I look for new experiences, but not this kind.
“: to bring (someone or something) back to a normal, healthy condition after an illness, injury, drug problem, etc.
b: to teach (a criminal in prison) to live a normal and productive life
c: to bring (someone or something) back to a good condition”
I hope it’s clear that it’s the first definition we’re dealing with today.
Forgive me for being dense, but I still didn’t get how that’s going to be done. So I searched for help and MedlinePlus, which is part of the U.S. National Library of Congress which, in turn, is part of the National Health Institutes, at https://medlineplus.gov/rehabilitation.html did just that.
“What happens in a rehabilitation program?
When you get rehabilitation, you often have a team of different health care providers helping you. They will work with you to figure out your needs, goals, and treatment plan. The types of treatments that may be in a treatment plan include
Assistive devices, which are tools, equipment, and products that help people with disabilities move and function
Cognitive rehabilitation therapy to help you relearn or improve skills such as thinking, learning, memory, planning, and decision making
Mental health counseling
Music or art therapy to help you express your feelings, improve your thinking, and develop social connections
Nutritional counseling
Occupational therapy to help you with your daily activities
Physical therapy to help your strength, mobility, and fitness
Recreational therapy to improve your emotional well-being through arts and crafts, games, relaxation training, and animal-assisted therapy
Speech-language therapy to help with speaking, understanding, reading, writing and swallowing
Treatment for pain
Vocational rehabilitation to help you build skills for going to school or working at a job
Depending on your needs, you may have rehabilitation in the providers’ offices, a hospital, or an inpatient rehabilitation center. In some cases, a provider may come to your home. If you get care in your home, you will need to have family members or friends who can come and help with your rehabilitation.”
Personally, I won’t need some of these such as cognitive rehabilitation, speech-language therapy, and vocational rehabilitation. Brain and speaking aren’t involved in pancreatic surgery and I’m retired. You may be in the same situation if you have rehabilitation or you may not. It’s a list that’s made unique for each patient. I’ve got to remind you here that I’m not a doctor; this is a lay person giving her opinion.
Hmmm, it seemed pretty clear that each type of surgery requires its own sort of rehabilitation. Now that we know what’s involved, let’s see who would be involved if you required rehabilitation after a surgery. WebMD at https://www.webmd.com/healthy-aging/rehab-after-surgery#1 offered a succinct, easy to understand answer.
“Who Works With You
Different experts help with different parts of your rehab. Some people who might be on your team:
Physiatrist. He’s a doctor who specializes in rehab. He tailors a plan to your needs and oversees the program to make sure it’s going well.
Physical therapist. He teaches you exercises to improve your strength and the range you have when you move your arm, leg, or whatever part of your body had the operation.
Occupational therapist. He helps you regain the skills you need for some basic activities in your everyday life. He might teach you how to cook meals, get dressed, shower or take a bath, and use the toilet. He’ll also show you how to use gadgets that can help you care for yourself more easily, such as a dressing stick or elastic shoelaces. Some occupational therapists will visit your home to make sure it’s safe and easy for you to get around.
Dietitian. He’ll help you plan healthy meals. If your doctor has told you to avoid salt, sugar, or certain foods after your surgery, the dietitian can help you find other choices.
Speech therapist. He helps with skills like talking, swallowing, and memory. Speech therapy can be helpful after surgery that affects your brain.
Nurses. They care for you if you’re staying for a few weeks or months in a rehab center. They may also come to your home to help track your recovery and help you with the transition to life back at home.
Psychologist or counselor. It’s natural to feel stressed out or depressed after your surgery. A mental health professional can help you manage your worries and treat any depression.
It can take many months to recover from an operation, but be patient. A lot depends on your overall health and the kind of procedure you had. Work closely with your rehab team and follow their instructions. Your hard work will pay off.”
Looking over the list, I won’t need a speech therapist and neither would you if you have some kind of kidney related surgery. I’m not so sure about a psychologist or counselor, either. I’m sort of thinking that going through chemotherapy and radiation treatments without one, I won’t need one after surgery. Then again, I’ve never had major surgery before and I’ve been told this is major major surgery. However, should I find myself in a position where my medical team and/or I feel I need counseling, I would not hesitate to ask for it… just as I’ve asked for help with the cancer.
Days 91 and beyond: $682 coinsurance per each “lifetime reserve day” after day 90 for each benefit period (up to 60 days over your lifetime).
Each day after the lifetime reserve days: all costs.
*You don’t have to pay a deductible for care you get in the inpatient rehabilitation facility if you were already charged a deductible for care you got in a prior hospitalization within the same benefit period. This is because your benefit period starts on day one of your prior hospital stay, and that stay counts towards your deductible.”
By now, you probably all know that I chose a clinical trial to treat my pancreatic cancer. But did you know that today, May 20th, is Clinical Trials Day? What’s that, you ask? Let’s find out together. According to The Association of Clinical Research Professionals (ACRP) at http://www.clinicaltrialsday.org/:
“WHY MAY 20?
Clinical Trials Day is celebrated around the world in May to recognize the day that James Lind started what is often considered the first randomized clinical trial aboard a ship on May 20, 1747.
HERE’S THE STORY
May, 1747.
The HMS Salisbury of Britain’s Royal Navy fleet patrols the English Channel at a time when scurvy is thought to have killed more British seamen than French and Spanish arms.
Aboard this ship, surgeon mate James Lind, a pioneer of naval hygiene, conducts what many refer to as the first clinical trial.
Acting on a hunch that scurvy was caused by putrefaction of the body that could be cured through the introduction of acids, Lind recruited 12 men for his ‘fair test.’…
Without stating what method of allocation he used, Lind allocated two men to each of six different daily treatments for a period of fourteen days. The six treatments were: 1.1 litres of cider; twenty-five millilitres of elixir vitriol (dilute sulphuric acid); 18 millilitres of vinegar three times throughout the day before meals; half a pint of sea water; two oranges and one lemon continued for six days only (when the supply was exhausted); and a medicinal paste made up of garlic, mustard seed, dried radish root and gum myrrh.…
Those allocated citrus fruits experienced ‘the most sudden and good visible effects,’ according to Lind’s report on the trial.
Though Lind, according to The James Lind Library, might have left his readers ‘confused about his recommendations’ regarding the use of citrus in curing scurvy, he is ‘rightly recognized for having taken care to “‘compare like with like’’, and the design of his trial may have inspired ‘and informed future clinical trial design.'”
I’ve written about James Lind before, so you may want to re-read the 8/20/18 blog to read more about him and his experiments.
Time travel to 2019 with me, if you will, to read what Antidote.Me has to offer in the way of Chronic Kidney Disease Clinical Trials.
****
Headline: Chronic Kidney Disease Research: How to Get Involved
By Nancy Ryerson
May 20 is Clinical Trials Day. Every year, patient advocates and research groups participate to raise awareness of how clinical trial participation drives research progress. You may know that new treatments for Chronic Kidney Disease (CKD) can’t move forward without clinical trial volunteers, but you may not know how to find active, relevant trials in your area.
Below, you’ll find answers to commonly asked questions about finding CKD clinical trials, including who can join, how to find trials, and the kinds of questions CKD research aims to answer.
How can I find Chronic Kidney Disease clinical trials near me?
There are currently 171 research studies for CKD looking for volunteers in the United States. All clinical trials are listed on ClinicalTrials.gov, but because the website was developed with researchers in mind rather than patients, it can be difficult for patients to navigate. Antidote is a clinical trial matching company that provides a patient-friendly clinical trial search tool to health nonprofits and bloggers, including this blog. With the Antidote tool, you can answer a few questions about your medical history and where you’d like to find a trial to receive a list of trials you may qualify for in your area. You can also sign up to receive alerts when new trials are added near you.
Who can join CKD clinical trials?
It’s a common misconception that clinical trials only need volunteers who have been recently diagnosed to take part. It’s also untrue that clinical trials are only a “last resort” for patients who have exhausted other options. In reality, clinical trials can be a care option for patients at any point after diagnosis. CKD trials need volunteers with mild, moderate, and severe kidney disease to participate in different trials. Some trials also look for patients with specific comorbidities, such as hypertension.
What does CKD research typically focus on?
Clinical trials for Chronic Kidney Disease (CKD) research potential new treatments to slow or stop CKD, as well as treat common conditions associated with CKD, such as anemia or hypertension.
CKD clinical trials aren’t limited to research into new drugs, either. For example, a kidney-friendly diet can make a significant difference in reducing kidney damage, and more research is needed into specific interventions that can help. Research studies are also looking into the impact exercise can have on CKD symptoms and progression.
Clinical trials may also be observational. These kinds of trials don’t test an intervention – a drug, diet, lifestyle change, etc. Instead, participants are divided into groups and observed for differences in outcome.
Do clinical trials always use a placebo?
In clinical trials, placebos – also known as “sugar pills” – help researchers understand the effectiveness of an experimental treatment. While they can be an important part of the research process, it’s also understandable that patients hope they won’t receive the placebo in a clinical trial.
If you’re considering taking part in a trial but you’re concerned about receiving a placebo, it’s important to know that not all trials use one. Many trials test a potential new treatment against the standard of care, for example. In some trials that use a placebo, everyone in the trial may receive the study drug at some point during the trial.
I don’t have time to participate in a clinical trial.
Time restraints are another reason many patients hesitate to participate in clinical trials. While some clinical trials may require weekly site visits, others may only ask participants to come in every month or so. Some trials may also offer virtual visits online or home visits to help reduce the number of trips you’ll need to take to get to a site. When you’re considering joining a clinical trial, ask the study team any questions you have about the trial schedule, reimbursement for travel, or anything else about participation.
Interested in finding a trial near you? Use the SlowItDownCKD trial search, powered by Antidote, to start your search. (Gail here: It’s at the bottom right hand side of the blog roll.)
Ladies and Gentleman, start your motors! I hope you find just the right CKD Clinical Trial for you.
As most of you know, I am extremely protective of my kidneys. When I was first diagnosed with Chronic Kidney Disease 11 years ago, my eGFR was only 39. Here’s a quick reminder of what the eGFR is from my first CKD book, What Is It and How Did I Get It? Early Stage Chronic Kidney Disease:
“GFR: Glomerular filtration rate [if there is a lower case ‘e’ before the term, it means estimated glomerular filtration rate] which determines both the stage of kidney disease and how well the kidneys are functioning.”
39. That’s stage 3B, the lower part of stage 3B. During the intervening 11 years, I’ve been able to raise it to 50 (and sometimes higher for short periods) via vigorously following the renal diet, exercising, avoiding stress as much as possible, maintaining adequate sleep, and paying strict attention to the medications prescribed for me. While the medications were the ones I had been taking for high blood pressure prior to being diagnosed with CKD, they worked in my favor.
This excerpt from The National Center for Biotechnology Information (NCBI) part of the United States National Library of Medicine (NLM), a branch of the National Institutes of Health (NIH) at https://www.ncbi.nlm.nih.gov/books/NBK492989/ will explain why:
“The decision of whether to reduce blood pressure levels in someone who has chronic kidney disease will depend on
how high their blood pressure is (when untreated),
whether they have diabetes, and
how much protein is in their urine (albumin level).
A person with normal blood pressure who doesn’t have diabetes and hardly has any albumin in their urine will be able to get by without using any blood-pressure-lowering medication. But people who have high blood pressure, diabetes or high levels of albumin in their urine are advised to have treatment with ACE inhibitors (angiotensin-converting enzyme inhibitors) or sartans (angiotensin receptor blockers). In people who have diabetes, blood-sugar-lowering medication is also important.”
When I was first diagnosed with pancreatic cancer early last month, it changed my medical priorities. With my nephrologist’s blessing, my primary focus was the cancer… not my kidneys. It took constant reminders to myself not to be so quick to say no to anything that I thought would harm my kidneys. In other words, to those things I’d been saying no to for the last 11 years.
For example, once diagnosed with CKD, I ate very little protein keeping to my five ounce daily limitation. Not anymore. Protein is needed to avoid muscle wasting during chemotherapy with a minimum requirement of eight ounces a day. I even tried roast beef and other red meats. After 11 years, they no longer agreed with me so I eat ground turkey, chicken, cheese, and am considering soy.
Another change: I preferred not to eat carbohydrates, but was warned not to lose weight if I could help it. All of a sudden I’m eating Goldfish, bread, and pasta. I can’t say that I’m enjoying them, but I am keeping my weight loss to a minimum. Other limitations like those on potassium and phosphorous have also gone by the wayside. I’ve eaten every childhood favorite, foods that I’ve avoided for the last 11 years, and anything that might look tempting in the last month, but none of them really taste that good. I like the foods on the renal diet now.
Oh, the only thing I have not increased is salt. My daughter takes me to my chemotherapy sessions. There’s a Jewish style restaurant across the street and we showed up early one day. I wanted to try a toasted bagel with butter, the way I ate it before CKD. The damned thing was salty! I hadn’t expected that.
Back to chemo and my kidneys. I admit it. I was nervous. What was this combination of poisons going to do to my kidneys? If it was so caustic that I had to have a port in place so that it wouldn’t be injected directly into my veins for fear of obliterating them, what about my kidneys?
I anxiously awaited my first Comprehensive Blood Panel, the blood test that includes your GFR. Oh, oh, oh! My kidney function had risen to 55 and my creatinine had lowered to 1.0. Let me explain just how good this was.
“Creatinine. Creatinine is a waste product from the normal breakdown of muscles in your body. Your kidneys remove creatinine from your blood. Providers use the amount of creatinine in your blood to estimate your GFR. As kidney disease gets worse, the level of creatinine goes up.”
Yet, mine went down. How? I asked and it was explained that all the hydration used to clear my veins of the caustic chemotherapy had worked this magic. I had two hours of hydration before the chemo-therapy itself, two hours afterward, and another two hours the next day. My kidneys had never been this hydrated!
But wait, there’s more. I have diabetes. The pancreas is the organ that produces insulin. Could my diabetes be from the tumor blocking the production of insulin by my pancreas? I truly don’t know, but my glucose level is within the standard range for the first time since I’ve been diagnosed with diabetes.
Would I recommend chemotherapy to raise your GFR, and lower your creatinine and your glucose level? Of course not. But I am feeling so very lucky that my kidneys are not coming to any harm during the chemotherapy necessary to save my life. I can’t begin to tell you how relieved I am.
National Kidney Month is just flying by. This is actually the last week and I doubt I’ll be able to post the rest of the 1in9 chapter before next month. But then again, it’s always Kidney Month for those of us with Chronic Kidney Disease. By the way, thank you to the reader who made it a point of telling me she can’t wait to read the rest of the chapter. Sooooo, let’s get started!
***
Nephrologist switch. The new one was much better for me. He explained again and again until I understood and he put up with a lot of verbal abuse when this panicky new patient wasn’t getting answers as quickly as she wanted them. Luckily for me, he graciously accepted my apology.
After talking to the nephrologist, I began to realize just how serious this disease was and started to wonder why my previous nurse practitioner had not caught this. When I asked her why, she responded, “It was inconclusive testing.” Sure it was. Because she never ordered the GFR tested; that had been incidental! I feel there’s no sense crying over spilled milk (or destroyed nephrons, in this case), but I wonder how much more of my kidney function I could have preserved if I’d known about my CKD earlier.
According to the Mayo Clinic, there are 13 early signs of chronic kidney disease. I never experienced any of them, not even one. While I did have high blood pressure, it wasn’t uncontrollable which is one of the early signs. Many, like me, never experienced any noticeable symptoms. Unfortunately, many, like me, may have had high blood pressure (hypertension) for years before CKD was diagnosed. Yet, high blood pressure and diabetes are the two leading causes of CKD. I find it confusing that uncontrollable high blood pressure may be an early sign of CKD, but hypertension itself is the second leading cause of CKD.
Here’s the part about my researching. I was so mystified about what was happening and why it was happening that I began an extensive course of research. My nephrologists did explain what everything meant (I think), but I was still too shocked to understand what they were saying. I researched diagnoses, descriptions of tests, test results, doctors’ reports, you name it. Slowly, it began to make sense, but that understanding only led to more questions and more research.
You’ve probably already guessed that my world changed during that first appointment. I began to excuse myself for rest periods each day when I went back East for a slew of family affairs right after. I counted food groups and calories at these celebrations that summer. And I used all the errand running associated with them as an excuse to speed walk wherever I went and back so I could fit in my exercise. Ah, but that was just the beginning.
My high blood pressure had been controlled for 20 years at that time, but what about my diet? I had no clue there was such a thing as a kidney diet until the nutritionist explained it to me. I’m a miller’s granddaughter and ate anything – and I do mean anything – with grain in it: breads, muffins, cakes, croissants, all of it. I also liked lots of chicken and fish… not the five ounces per day I’m limited to now.
The nutritionist explained to me how hard protein is on the kidneys… as is phosphorous… and potassium… and, of course, sodium. Out went my daily banana—too high in potassium. Out went restaurant burgers—larger than my daily allowance of protein. Chinese food? Pizza? Too high in sodium. I embraced an entirely new way of eating because it was one of the keys to keeping my kidneys functioning in stage 3.
I was in a new food world. I’d already known about restricting sodium because I had high blood pressure, but these other things? I had to keep a list of which foods contain them, how much was in each of these foods, and a running list of how much of each I had during the day so I knew when I reached my limit for that day.
Another critical piece of slowing down CKD is medication. I was already taking meds to lower my blood pressure when I was first diagnosed with CKD. Two more prescriptions have been added to this in the last decade: a diuretic that lowers my body’s absorption of salt to help prevent fluid from building up in my body (edema), and a drug that widens the blood vessels by relaxing them. I take another drug for my brand new diabetes. (Bye-bye, sugars and most carbs.) The funny thing is now my favorite food is salad with extra virgin olive oil and balsamic vinegar. I never thought that would happen: I was a chocoholic!
Exercise, something I loved until my arthritis got in the way, was also important. I was a dancer. Wasn’t that enough? Uh-uh, I had to learn about cardio and strength training exercise, too. It was no longer acceptable to be pleasantly plumb. My kidneys didn’t need the extra work. Hello to weights, walking, and a stationary bike. I think I took sleep for granted before CKD, too, and I now make it a point to get a good night’s sleep. A sleep apnea device improved my sleep—and my kidney function rose.
I realized I needed to rest, too. Instead of giving a lecture, running to an audition, and coming home to meet a deadline, I slowly started easing off until I didn’t feel like I was running on empty all the time. The result was that I ended up graciously retiring from both acting and teaching at a local college, which gave me more time to work on my CKD awareness advocacy.
***
There’s so much more to tell you about my personal CKD journey… and you’ll read more of it next week. Although, I should remind you that the entire book is available in print and digital on both Amazon.com and B&N.com, just as the entire SlowItDownCKD series of books is.
Tomorrow is Christmas and a Merry Christmas to those of you who celebrate. The day after Christmas Kwanzaa begins, so a Happy Kwanzaa to those of you who celebrate. But back to Christmas right now: today’s blog is a present to a reader who joined me way back when I first started blogging and has since become a close online friend.
You see, her creatinine is rising but she’s barely eating and – since she has multiple physical conditions – can’t exercise. She’s flummoxed and so was I because food and muscle waste are the two usual causes of rising creatinine levels in the blood. I decided to try to help her sort this out now even though she’ll be seeing her nephrologist right after the New Year.
A good place to start is always at the beginning. By this, I wonder if I mean the beginning of my Chronic Kidney Disease awareness advocacy as the author of What Is It and How Did I Get It? Early Stage Chronic Kidney Disease and the blog or if I mean the basics about creatinine. Let’s combine them all. The following definition is from the book which became the earliest blogs:
“Creatinine clearance: Compares the creatinine level in your urine with that in your blood to provide information about your kidney function”
Hmmm, that didn’t exactly work. Let’s try again. Bingo! It was in SlowItDownCKD 2014,
“Creatinine: chemical waste product that’s produced by our muscle metabolism and to a smaller extent by eating meat. {MayoClinic.org}”
“Protein intake from the diet is important during the progression of chronic kidney disease and also when you commence dialysis. The protein we eat is used for tissue repair and growth. Any unused protein is broken down into waste products, including urea and creatinine. As your kidneys are unable to excrete urea and creatinine properly, they build up in your blood and cause symptoms such as nausea and loss of appetite.
By eating large amounts of protein foods e.g. meat, fish, chicken, eggs, cheese, milk and yoghurt before commencing dialysis [Me here, that means those of us who are pre-dialysis like me], you will affect the buildup of urea and creatinine in your blood. An appropriate daily intake of protein should be advised by your dietician.
However, once dialysis treatment has commenced it is important to make sure that your body is getting enough protein to prevent malnutrition. Some of your stores of protein are lost during the haemodialysis and CAPD sessions. How much protein you need depends on your body size and is specific to each individual.”
And the ‘muscle metabolism’ in our definition? This deals with the way muscles use energy. The waste product of this process is creatinine.
“Strenuous exercise, such as weight training or resistance exercise, may cause high creatinine levels.
Muscle activity produces creatinine; the more the muscles work, the more creatinine is in the blood. While regular exercise is essential for good health, overexertion can cause the creatinine levels in the blood to spike.
A 2012 study noted that intense exercise increased creatinine levels in the bloodstream temporarily. It may be best for people to avoid strenuous activity until they have completed any treatment for the cause of the high creatinine levels.
However, people should not avoid exercise altogether, except in some extreme circumstances.
To maintain their exercise regimen, people who like weight training or resistance exercises could switch to yoga and body weight exercises during treatment. People who prefer cardio exercises, such as running or cycling, could consider changing to walking or swimming.”
“Kidney diseases or disorders can lead to high creatinine levels. Since the kidneys are the filters of wastes from the bloodstream, kidney damage means that there will be a buildup of creatinine beside other waste products in the body. Kidney conditions such as glomerulonephritis, acute tubular necrosis, kidney infection (pyelonephritis) and kidney failure can cause high creatinine levels. Reduced blood flow to the kidneys can also have a similar effect.
Other causes of elevated creatinine levels in blood include shock, dehydration, and congestive heart failure. These conditions lead to a reduction in blood flow to the kidneys, which interferes with their normal functions. High blood pressure, diabetic neuropathy, muscular dystrophy, rhabdomyolysis, eclampsia, and preeclampsia can also cause elevated serum creatinine.
In case a patient with renal dysfunction gets an infection like pneumonia, urinary tract infection, intestinal infection, or a cold, the creatinine level may rise within a short time.
Urine abnormalities such as long-term hematuria and proteinuria can also lead to high creatinine levels.
Taking drugs that have renal toxicity properties can also raise the levels of creatinine in the bloodstream. Such medications include chemotherapy drugs, ACE inhibitors, and NSAIDs like aspirin and ibuprofen among others.”
They also included excessive exercise, too much protein in the diet, fatigue, and inadequate rest.
I noticed each site I looked at mentioned that creatinine increase could be temporary. Perhaps a re-test is in order for my friend.
I know you’re already asking why she was surprised to find this on her lab report. She already has CKD which could be a cause of high creatinine levels. What worried her is that they are rising. Is her CKD getting worse? Or did she neglect to get adequate rest (as one possibility) before this particular blood test?
I can’t answer that since I’m not a doctor, although I hope I’ve been able to alleviate her worry until she gets to go to her nephrologist next week. Here’s hoping this was a welcome Christmas present, my friend.
The holiday season is upon us full strength right now, but you have Chronic Kidney Disease. You don’t need the stress associated with the holiday season. The National Kidney Fund at https://www.kidney.org/atoz/content/Stress_and_your_Kidneys explains why:
“As the blood filtering units of your body, your kidneys are prone to problems with blood circulation and blood vessels. High blood pressure and high blood sugar can place an additional strain or burden on your kidneys. People with high blood pressure and diabetes are at a higher risk for kidney disease. People with kidney disease are at higher risk for heart and blood vessel disease. If you already have heart and blood vessel disease and kidney disease, then the body’s reactions to stress can become more and more dangerous. Therefore, whether your goal is to prevent heart and/or kidney disease, or improve your health while living with heart and/or kidney disease, managing stress is an important part of maintaining your overall health.”
So what’s a CKD patient to do? First, you need to identify that you are stressed. In an article on caretaker stress at https://www.davita.com/education/ckd-life/caregiver/caregiver-stress-and-chronic-kidney-disease, DaVita outlined some of the symptoms. These are the same whether you’re the patient or the caretaker. I happen to be both a CKD patient and my Alzheimer’s husband’s caretaker, although we call me his care partner as suggested by the Alzheimer’s Association.
Physical signals
Inability to sleep or sleeping too much
Weight gain or loss
Feeling tired all the time
Change in posture—walking with your head down or with a stooped posture
Withdrawing from usual activities and relationships
Quitting or changing jobs frequently
Becoming more impulsive and over-reacting to things
Using alcohol or drugs to feel better
Uh-oh, I recognize quite a few of these in myself. How about you?
Today is the last day of the eight day Chanukah celebration for us and all of you who celebrate this holiday. We usually throw a blowout party for anywhere from 30 to 50 people. But just a couple of months ago, we hosted a blowout pre-wedding potluck party for my daughter and her fiancé … and it was wonderful. Yet, it was clear that we can no longer handle undertaking such large parties. I had expressed my doubts last year about how long we’d be able to keep up the Chanukah party.
I was getting more and more stressed dealing with Bear’s medical issues and my own and then the party, so I did what I consider the logical thing to do, I delegated. We’ll still have the party, but a friend of my daughter’s will be hosting it. Instead of assigning different foods to specific guests, we’ve asked them to let us know what they’re be bringing. No prepping of the house (Shiloh sheds an entire other dog every few days) and no post party clean up. More importantly, no stress. I just bring the religious articles necessary and toss in a batch of cranberry chicken as my food contribution. Easy-peasy.
My very capable neighbor came in with cookies she’d just baked the other day. She knows about Bear’s sweet tooth. We started chatting as we’re wont to do and she brought up the point that she finds delegating stressful. Amy wants to make sure whatever it is that’s being delegated is done and done well, so she has to be careful about who she choices. I see her point, but I think that if you know your friends and family and how responsible (or not) each is, this shouldn’t be a problem.
But enough about me. What else can you do to reduce your stress at this time of year?
“For people with kidney disease, even eating normal amounts of food puts stress on their kidneys. If you consume large amounts of carbohydrates, protein or fat the stress on an overworked, half functioning kidney will get even worse and can accelerate your kidney dysfunction.”
Exercise increases your overall health and your sense of well-being, which puts more pep in your step every day. But exercise also has some direct stress-busting benefits.
It pumps up your endorphins. Physical activity helps bump up the production of your brain’s feel-good neurotransmitters, called endorphins. Although this function is often referred to as a runner’s high, a rousing game of tennis or a nature hike also can contribute to this same feeling.
It’s meditation in motion. After a fast-paced game of racquetball or several laps in the pool, you’ll often find that you’ve forgotten the day’s irritations and concentrated only on your body’s movements.
As you begin to regularly shed your daily tensions through movement and physical activity, you may find that this focus on a single task, and the resulting energy and optimism, can help you remain calm and clear in everything you do.
It improves your mood. Regular exercise can increase self-confidence, it can relax you, and it can lower the symptoms associated with mild depression and anxiety. Exercise can also improve your sleep, which is often disrupted by stress, depression and anxiety. All of these exercise benefits can ease your stress levels and give you a sense of command over your body and your life.
Of course, you could give yourself permission to curl up with a good book for half an hour or so. You might like Portal in Time or Sort of Dark Places for sheer escapism or any of the SlowItDownCKD series (including What Is It and How Did I Get It? Early Stage Chronic Kidney Disease) for edifying yourself. Oh, the shameless self-promotion here! All are available on Amazon although,personally, if I’m stressed, I want pure escapism.
Sorry Batman, not yours. I’m writing about Chronic Kidney Disease and diabetes. For a decade, I’ve been told diabetes is the number one cause of CKD. Got it… and (as you know) CKD. Then I learned that CKD can cause diabetes. Ummm, okay, I guess that sort of makes sense. And then, oh my, I developed diabetes. But how? I’d never questioned how that worked before, but I certainly did now.
Let’s go back to the beginning here. First of all, what is diabetes? I included this information in SlowItDownCKD 2013:
‘Diabetes, often referred to by doctors as diabetes mellitus, describes a group of metabolic diseases in which the person has high blood glucose (blood sugar), either because insulin production is inadequate, or because the body’s cells do not respond properly to insulin, or both. Patients with high blood sugar will typically experience polyuria (frequent urination), they will become increasingly thirsty (polydipsia) and hungry (polyphagia).’”
Guilty on all three counts as far as symptoms. It gets worse. I uncovered this fact in SlowItDownCKD 2014:
‘The kidneys are another organ that is at particular risk of damage as a result of diabetes and the risk is again increased by poorly controlled diabetes, high blood pressure and cholesterol.’”
This is getting more and more complicated. But again, how is diabetes damaging my kidneys?
It seemed to me that I had just posted a fact about this on SlowItDownCKD’s Facebook page, so I checked. Yep, I did on September 7th.
“Did you know that high glucose levels can make your red blood cells stiffen? This hinders your blood circulation.”
Hmmm, so red blood cells compose one quarter of your blood and high glucose can make them stiffen. To me, that means a quarter of your blood will be working against you. Not what we need… especially when we’re already dealing with Chronic Kidney Disease.
Back to my original question (again): How do high glucose levels affect the kidneys?
Blood vessels inside your kidneys. The filtering units of the kidney are filled with tiny blood vessels. Over time, high sugar levels in the blood can cause these vessels to become narrow and clogged. Without enough blood, the kidneys become damaged and albumin (a type of protein) passes through these filters and ends up in the urine where it should not be.
Nerves in your body. Diabetes can also cause damage to the nerves in your body. Nerves carry messages between your brain and all other parts of your body, including your bladder. They let your brain know when your bladder is full. But if the nerves of the bladder are damaged, you may not be able to feel when your bladder is full. The pressure from a full bladder can damage your kidneys.
Urinary tract. If urine stays in your bladder for a long time, you may get a urinary tract infection. This is because of bacteria. Bacteria are tiny organisms like germs that can cause disease. They grow rapidly in urine with a high sugar level. Most often these infections affect the bladder, but they can sometimes spread to the kidneys.
I would say I’m heart… uh, kidney…broken about this development, but the truth is I’m not. I don’t like it; I don’t want it, but I can do something about it. I’d already cut out complex carbs and sugar laden foods in an abortive attempt to lose weight for my health. Well, maybe my daughter’s wedding on October 6th had something to do with that decision, too.
The point is, I’ve started. I’m aware of the carbohydrates in food and I’m learning how to control my intake of them… just as I’m aware that I have to break in the shoes for the wedding. Something new has to be gotten used to. I’ve had a head start.
“When you eat foods containing carbohydrates, your digestive system breaks down the sugars and starches into glucose. Glucose is one of the simplest forms of sugar. Glucose then enters your bloodstream from your digestive tract and raises your blood glucose levels. The hormone insulin, which comes from the pancreas or from insulin shots, helps cells throughout your body absorb glucose and use it for energy. Once glucose moves out of the blood into cells, your blood glucose levels go back down.”
If you’ve got diabetes, your body either is not producing enough insulin or not interacting well with the insulin it is producing. Measuring my blood sugar levels when I awaken in the morning has shown me that when I’m sleeping – when I cannot help my blood sugar levels come down by eating protein or exercising, even in my dreams – is when I have the highest blood sugar. During the day I can keep it under control.
And that’s where my medication comes in. The usual – Metformin – can cause nausea, which I deal with more often than not, so that was out. However, a new medication on the market just might do the trick. It’s only been a few days, but I do notice my blood sugar upon waking is getting lower each day. This medication is not a panacea. I still have to be careful with my food, exercise daily, and sometimes counteract a high carb food with a protein. I’m not there yet, but I’m learning.
Loads of good things have been happening in my family lately, among them a couple of marriages. That, of course, brings new people into the family. There’s always that obligatory meet-the-new-in-laws dinner. At one of these, a just added family member mentioned that she only had one kidney. Then she asked me what that means as far as Chronic Kidney Disease… and I didn’t know. Today’s blog is for her.
When a person has only one kidney or one working kidney, this kidney is called a solitary kidney. People born with kidney dysplasia have both kidneys; however, one kidney does not function (top right). When a kidney is removed surgically due to disease or for donation, both the kidney and ureter are removed (bottom right).
Well that was pretty straight forward. I wondered if she should be taking any kind of special cautions. According to the National Center for Biotechnology Information of the U.S. National Library of Medicine, National Institutes of Health, PubMed at https://www.ncbi.nlm.nih.gov/pubmed/16985610,
Removal of one kidney leads to structural and functional changes by the remaining kidney, including increased filtration of the remaining glomeruli. These functional changes have generally been considered beneficial because they mitigate the reduction in the total glomerular filtration rate that would otherwise occur, but experimental evidence suggests that these changes may have an adverse effect on the remaining kidney.
If having a single kidney does affect your health, the changes are likely to be so small and happen so slowly that you won’t notice them. Over long periods of time, however, these gradual changes may require specific measures or treatments. Changes that may result from a single kidney include the following:
High blood pressure. Kidneys help maintain a healthy blood pressure by regulating how much fluid flows through the bloodstream and by making a hormone called renin that works with other hormones to expand or contract blood vessels. Many people who lose or donate a kidney are found to have slightly higher blood pressure after several years.
Proteinuria. Excessive protein in the urine, a condition known as proteinuria, can be a sign of kidney damage. People are often found to have higher-than-normal levels of protein in their urine after they have lived with one kidney for several years.
Reduced GFR. The glomerular filtration rate (GFR) shows how efficiently your kidneys are removing wastes from your bloodstream. People have a reduced GFR if they have only one kidney.
In the nephron …, tiny blood vessels intertwine with urine-collecting tubes. Each kidney contains about 1 million nephrons.
You can have high blood pressure, proteinuria, and reduced GFR and still feel fine. As long as these conditions are under control, they will probably not affect your health or longevity. Schedule regular checkups with your doctor to monitor these conditions.
Wait a minute! Those are also the effects of Chronic Kidney Disease. And as you read on, you’ll see that the precautions are the same as those for someone who already has CKD.
Your doctor should monitor your kidney function by checking your blood pressure and testing your urine and blood once a year.
Normal blood pressure is considered to be 120/80 or lower. You have high blood pressure if it is over 140/90. People with kidney disease or one kidney should keep their blood pressure below 130/80. Controlling blood pressure is especially important because high blood pressure can damage kidneys.
Your doctor may use a strip of special paper dipped into a little cup of your urine to test for protein. The colour of the “dipstick” indicates the presence or absence of protein. A more sensitive test for proteinuria involves laboratory measurement and calculation of the protein-to-creatinine ratio. A high protein-to-creatinine ratio in urine (greater than 30 milligrams of albumin per 1 gram of creatinine) shows that kidneys are leaking protein that should be kept in the blood.
… scientists have discovered that they can estimate a person’s GFR based on the amount of creatinine in a small blood sample. The new GFR calculation uses the patient’s creatinine measurement along with weight, age, and values assigned for sex and race. …. If your GFR stays consistently below 60, you are considered to have chronic kidney disease.
Controlling Blood Pressure
If your blood pressure is above normal, you should work with your doctor to keep it below 130/80. Great care should be taken in selecting blood pressure medicines for people with a solitary kidney. Angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) are two classes of blood pressure medicine that protect kidney function and reduce proteinuria. But these medicines may be harmful to someone with renal artery stenosis (RAS), which is the hardening of the arteries that enter the kidneys. Diuretics can help control blood pressure by removing excess fluid in the body. Controlling your blood pressure may require a combination of two or more medicines, plus changes in diet and activity level.
Eating Sensibly
Having a single kidney does not mean that you have to follow a special diet. You simply need to make healthy choices, including fruits, vegetables, grains, and low-fat dairy foods. Limit your daily salt (sodium) intake to 2,000 milligrams or less if you already have high blood pressure. Reading nutrition labels on packaged foods to learn how much sodium is in one serving and keeping a sodium diary can help. Limit alcohol and caffeine intake as well.
Avoid high-protein diets. Protein breaks down into the waste materials that the kidneys must remove, so excessive protein puts an extra burden on the kidneys. Eating moderate amounts of protein is still important for proper nutrition. A dietitian can help you find the right amount of protein in your diet.
Avoiding Injury
…. Having a solitary kidney should not automatically disqualify you from sports participation. Children should be encouraged to engage in some form of physical activity, even if contact sports are ruled out. Protective gear such as padded vests worn under a uniform can make limited contact sports like basketball or soccer safe. Doctors, parents, and patients should consider the risks of any activity and decide whether the benefits outweigh those risks.
I am happy to say I think our new relative is going to find this a comforting blog. I know I did.
Oh, talking about one. I have one desk copy of the now retired The Book of Blogs: Moderate Stage Chronic Kidney Disease, Part 2 left. Leave a comment if you’d like to have it. All I ask is that you not have received a free book from me before.
I’m not a joiner. I’ve never been one. That’s why I was so surprised that I joined the American Association of Kidney Patients… and even more surprised to find myself attending this year’s conference in Tampa Bay, Florida. Readers had been suggesting I do so for years, but I’m not a joiner. Let’s change that; I wasn’t a joiner. The AAKP conference made the difference.
What’s that you ask? Of course, you need to know what they are. This is from their website at https://aakp.org/,
“THE INDEPENDENT VOICE OF KIDNEY PATIENTS SINCE 1969™
The American Association of Kidney Patients is dedicated to improving the quality of life for kidney patients through education, advocacy, patient engagement and the fostering of patient communities.
Education
The American Association of Kidney Patients (AAKP) is recognized as the leader for patient-centered education – continually developing high quality, professionally written, edited and reviewed educational pieces covering every level of kidney disease.
Advocacy
For nearly 50 years, AAKP has been the patient voice – advocating for improved access to high-quality health care through regulatory and legislative reform at the federal level. The Association’s work has improved long term outcomes in both quality of health and the ability for patients and family members affected by kidney disease to lead a more productive and meaningful life.
Community
AAKP is leading the effort to bring kidney patients together to promote community, conversations and to seek out services that help maximize patients’ everyday lives.
An IRS registered, Sec. 501(C)(3) organization, AAKP is governed by a Board of Directors. The current board is comprised of dialysis patients, chronic kidney disease patients, [Me here: You did notice ‘chronic kidney disease patients,’ right?] transplant recipients, health care professionals and members of the public concerned with kidney disease. The board and membership are serviced by a staff of five employees under the direction of Diana Clynes, Interim Executive Director, at the AAKP National Office located in Tampa, Florida.”
What’s not mentioned here is that the organization was started by only six patients. I find that astounding, but I’ll let them explain their history:
“Founded by Patients for Patients
King County Hospital, New York
The American Association of Kidney Patients (AAKP) has a rich history in patient advocacy and kidney disease education. AAKP started in 1969 with six dialysis patients at King County Hospital in Brooklyn, New York. They wanted to form an organization that would elevate the kidney patient voice in national health care arena, provide patients with educational resources to improve their lives and give kidney patients and their family members a sense of community. They met twice a week in the hospital ward and while hooked up to primitive dialysis machines for 12 to 18 hours at a time they brainstormed, researched and eventually formed AAKP.
The group originally called themselves NAPH (National Association of Patients on Hemodialysis, which later changed to AAKP). AAKP joined forces with other patient groups to fight for the enactment of the Medicare End-Stage Renal Disease (ESRD) Program, testifying before congressional committees, seeking public support and creating a newsletter (the forerunner of today’s AAKP RENALIFE) to keep everyone informed. This effort was crowned with success in 1972 when Congress enacted the program that continues to provide Medicare funding for dialysis and kidney transplantation.
After winning the initial and critical battle for the Medicare ESRD Program, AAKP turned its attention to other important issues — the need to establish a secure national organization to preserve the visibility and influence of patients with Congress and to develop national, educational and supportive programs.
Today & Beyond
AAKP has grown into a nationally recognized patient organization that reaches over 1 million people yearly. It remains dedicated to providing patients with the education and knowledge necessary to ensure quality of life and quality of health.”
This former non-joiner has found her association. I originally avoided the conferences because I thought they would be focused only on dialysis and transplant patients. Boy, was I ever wrong. Here are some of the outbreak (small group) sessions that dealt with other aspects of kidney disease:
Social Media (You’re right: I signed up for that one right away since I identify as a CKD awareness advocate.)
Dental Health
How Kidney Disease Impacts Family Members
Managing the Early Stage of CKD
Understanding Clinical Trials
Treatment Options
Staying Active
Veterans Administration
Caregiver’s Corner
Living Well with Kidney Disease
Avoid Infections
Of course, there were many outbreak sessions for dialysis and transplant patients as well. And there were two opportunities to lunch with experts. That’s where I tentatively learned about governmental aspects of our disease. There were opportunities to learn about nutrition, medications, working, and coping. I’ve just mentioned a few of the 50 different topics discussed.
The general sessions, the ones everyone attended, informed us of what the government’s national policy had to do with kidney disease, legislation, nutrition, patient centered care, and innovation in care (Keep an eye out for Third Kidney, Inc.’s August guest blog.).
I have not covered even half of what was offered during the conference. Did I mention renal friendly food was available and you could dialyze near the hotel if need be? The exhibitors went beyond friendly and explaining their products to being interested in who you were and why you were there. This was the most welcoming conference I’d been to in decades.
AAKP President Paul Conway summed up my feelings about the conference when he was interviewed by The Tampa Bay Times on the last day of the conference,
“This meeting is a way for us to bring patients together and educate them on trends that could affect their own health.”
I met so many others who have kidney disease and so many others who advocate for different types of kidney disease and patients’ rights. I was educated about so many areas, especially those I previously had known nothing about, for example, legislation. It was like coming home. Would I attend again? You bet’cha. Would I urge you to attend? At the risk of being redundant, you bet’cha.
I was so excited about AAKP that I almost didn’t leave myself enough space to tell you about yet another freebie. The Book of Blogs: Moderate Chronic Kidney Disease, Part 1 is no longer in print since it has been divided into SlowItDownCKD 2011 and SlowItDownCKD 2012. But I still have a desk copy. Let me know if you’d like it. My only restriction is that you have not received a free book from me before.
When I was a little girl, I liked to listen to my father whistle ‘All of Me,’ written by Marks and Simon in 1931 when Charlie, my father, was just 16. Only a few years later, it became a sort of love language for my mother and him. Enter a former husband of my own and my children. When my folks visited from Florida and my then husband’s side of the family journeyed over to Staten Island from Brooklyn to visit them, they all sang the song with great emotion. (By then, Bell’s palsy had robbed my father of the ability to whistle.)
To this day, I start welling up when I hear that song. But then I started thinking about the lyrics:
“All of me
Why not take all of me?”
Suddenly, it popped. For us, those with chronic kidney disease, it should be:
“All of us
Why not take all of us?”
For research purposes. To “speed up health research breakthroughs.” For help in our lifetime. To spare future generations whatever it is we’re suffering… and not just for us, but for our children… and their children, too.
The National Institutes of Health has instituted a new research program for just that purpose, although it’s open to anyone in the U.S. over the age of 18 whether ill with any disease or perfectly healthy. While only English and Spanish are the languages they can accommodate at this time, they are adding other languages.
I’m going to devote most of the rest of this blog to them. By the way, I’m even more inclined to be in favor of this program because they launched on my first born’s birthdate: May 6. All of Us has its own inspiring welcome for you at https://launch.joinallofus.org/
This is how they explain who they are and what they intend to do:
“The goal is to advance precision medicine. Precision medicine is health care that is based on you as an individual. It takes into account factors like where you live, what you do, and your family health history. Precision medicine’s goal is to be able to tell people the best ways to stay healthy. If someone does get sick, precision medicine may help health care teams find the treatment that will work best.
To get there, we need one million or more people. Those who join will share information about their health over time. Researchers will study this data. What they learn could improve health for generations to come. Participants are our partners. We’ll share information back with them over time.”
You’ll be reading more about precision medicine, which I’ve written about before, in upcoming blogs. This is from All of Us’s website at https://www.joinallofus.org/en, as is most of the other information in today’s blog, and makes it easy to understand just what they are doing.
How It Works
Participants Share Data
Participants share health data online. This data includes health surveys and electronic health records. Participants also may be asked to share physical measurements and blood and urine samples.
Data Is Protected
Personal information, like your name, address, and other things that easily identify participants will be removed from all data. Samples—also without any names on them—are stored in a secure biobank.
Researchers Study Data
In the future, approved researchers will use this data to conduct studies. By finding patterns in the data, they may make the next big medical breakthroughs.
Participants Get Information
Participants will get information back about the data they provide, which may help them learn more about their health.
Researchers Share Discoveries
Research may help in many ways. It may help find the best ways for people to stay healthy. It may also help create better tests and find the treatments that will work best for different people.
I’m busy, too busy to take on even one more thing. Or so I thought. When I read the benefits of the program (above) and how easy it is to join (below), I realized I’m not too busy for this and it is another way to advocate for Chronic Kidney Disease awareness. So I joined and hope you will, too.
Benefits of Taking Part
Joining the All of Us Research Program has its benefits.
Our goal is for you to have a direct impact on cutting-edge research. By joining the program, you are helping researchers to learn more about different diseases and treatments.
Here are some of the benefits of participating in All of Us.
Better Information
We’re all human, but we’re not all the same. Often our differences—like age, ethnicity, lifestyle habits, or where we live—can reveal important insights about our health.
By participating in All of Us, you may learn more about your health than ever before. If you like, you can share this information with your health care provider.
Better Tools
The goal of the program is better health for all of us. We want to inspire researchers to create better tools to identify, prevent, and treat disease.
You may also learn how to use tools like mobile devices, cell phones and tablets, to encourage healthier habits.
Better Research
We expect the All of Us Research Program to be here for the long-term. As the program grows, the more features will be added. There’s no telling what we can discover. All thanks to participants like you.
Better Ideas
You’re our partner. And as such, you are invited to help guide All of Us. Share your ideas and let us know what works, and what doesn’t.
Oh, about joining:
Get Started – Sign Up
Here’s a quick overview of what you’ll need to do to join.
1
Create an Account
You will need to give an email address and password.
2
Fill in the Enrollment and Consent Forms
The process usually takes 18-30 minutes. If you leave the portal during the consent process, you will have to start again from the beginning.
3
Complete Surveys and More
Once you have given your consent, you will be asked to complete online health surveys. You may be asked to visit a partner center. There, you’ll be asked to provide blood and urine samples and have your physical measurements taken. We may also ask you to share data from wearables or other personal devices.
Before I leave you today, I have – what else? – a book give away. The reason? Just to share the joy that’s walked into my life lately. It’s easy to share the troubles; why not the joys? If you haven’t received one of my books in a giveaway before, all you have to do is be the first person to let me know you want this copy of SlowItDownCKD 2017.
I need to get back to that online health survey for All of Us now.
Again, and again you’ve heard me rant about why we, as CKD patients, are not diagnosed earlier so we can start treating our Chronic Kidney Disease with – at least – life style changes earlier. That could help us slow down the progression of decline in our kidney function. I maintain that if only my primary care physician had told me when he first noticed that 39% GFR, maybe I wouldn’t be in stage 3 of 5. Maybe those now on dialysis or searching for a transplant wouldn’t be in the position they are, either.
It looks like our doctors are starting to feel the same way. Thank goodness. As a CKD Awareness Advocate, I’ve met others with the same advocacy. Robin is a doctor who feels the same, and someone I consider a friend. When I read her article, I jumped at the chance to guest blog it since she has the understanding of the medicalese that can frustrate the rest of us. Without further ado, Dr. Robin Rose…
Doctor, doctor give me this news: Primary care and CKD
Everyone’s mind jumps right to end-stage renal disease and dialysis when kidney disease is mentioned, even among clinicians. By the time a patient needs dialysis, pathology has been smoldering, sometimes for prolonged periods of time. Nephrology gracefully manages later-stage kidney disease, but it seems the incipient cases remain in the shadows. In general practice, kidneys are often ignored.
What I want to know is this: How can we effectively forge a path between nephrology and primary care — take the reins and together harness the epidemic, starting early while the pathology of the disease may be more easily addressed?
Too many patients and too many of their primary care providers are simply unaware of renal status. The staggering number of stage 3 chronic kidney disease (CKD) cases dramatically dwindles by stage 4, and CKD exacerbates so many underlying pathologies. Morbidity leads to mortality, often without recognition of underlying kidney damage as the prominent culprit. With the worldwide nephrologist shortage, and clearly with the high cost of end-stage care, it may well be time to expand the renal education and early/moderate CKD clinical savvy in primary care.
Build CKD recognition
As a physician, I recognize pharmaceutical options as a small part of longitudinal CKD care. The point of early diagnosis is assisting patients with the arduous and necessary journey to lifestyle change. Primary care has embraced this supportive role for other diagnoses, such as cancer, diabetes, heart disease, etc. This type of synergistic/collaborative care — reinforcing specialist input, following each person with his or her myriad issues — is the perfect fit for CKD.
How do we communicate to make our generalist and specialist intent merge into one clear target — enhanced patient quality of life? How can we make this work — to commence having a serious problem-solving conversation?
The literature suggests early nephrologist involvement improves long-term outcomes. Proactive primary care offers longitudinal guidance for making the enormous lifestyle changes in diet, exercise, stress management, hydration, sleep and toxic exposures, while offering psychological counseling that is required to achieve such changes. The cross-over benefits for patients’ other diagnoses is well known.
This concept of primary care nephrology could unfold into clinical reality as a professional, collaborative cooperation. With the diagnostic refinement of the nephrologist, a primary care physician can guide patients with CKD with the balancing act of comorbidities, medication management and optimal kidney lifestyle.
Likewise, what this family physician recognizes as critically useful from the consulting nephrologist is the expert focus on pathology with a diagnosis and back-up. We must agree that things like diet, exercise, sleep, stress and toxins have longitudinal importance for our patients with CKD — important enough for the primary care physician to make time with motivated patients to assess and co-discover actionable adaptations. Comorbidities with time will certainly guide the process. The success of this requires supportive enthusiasm from the specialist.
Vision of collaboration
Here is an example: A 46-year-old perimenopausal working single mother, with a history 12 years prior of pregnancy-induced hypertension and diabetes, has moderate proteinuria and a creatinine of 1.2. A nephrology consult will crystallize her individual needs. A primary care plan will address medications, CKD lifestyle needs and illuminate the notable overlap of benefits for her other diagnoses.
During the course of four visits looking at her stress, relationship to food and exercise needs, she exhibits admirable motivation, paying attention to what and how she eats and enjoying a lunchtime walking program. Reinforcing these successes while addressing medications, diet, sleep, etc. every 3 months offers an opportunity to protect nephrons and proceed further in the adaptations needed.
At this time, nephrologists cannot assume this is taking place in all primary care settings. Primary care providers, guiding patients with CKD safely through commonplace medical scenarios — like infectious illnesses, traumatic injuries, surgeries, travel and stress — need to grasp a breadth of nephrology basics. Our patients with CKD are at increased risk of acute kidney injury. Astute protection means we save nephrons. This author would welcome renal rotations at all levels of medical training, with a facet of focus on longitudinal outpatient, early and moderate CKD care. This vision of collaboration, with a commitment to early diagnosis and intervention, offers the opportunity to learn how to guide patients to a less inflammatory lifestyle.
The urgency is there. Can we talk?
For more information:
Robin Rose, MD, is a semi-retired family physician with a long-time interest in chronic illness and the role of lifestyle, with an interest in incipient and moderate CKD as a current focus. She lives in Molokai, Hawaii.
Disclosure: Rose reports no relevant financial disclosures.
Here’s a suggestion. Why not bring this article to your primary care physician? It could be that renal disease has never really crossed his mind despite the fact that 90% of the 31 million people in the U.S. who have CKD are unaware they do. You may not benefit from this – already having been diagnosed – but the next patient may… and the one after that… and the one after that…keep going.
Are you ready for the most important sentence in the mytherapyapp.com guest blog which was published on World Kidney Day on March 8th? This was the day that celebrated Chronic Kidney Disease and Women’s Health – during March’s National Kidney Month and National Women’s Month. Well then, here it is, along with the rest of the mytherapyapp.com guest blog.
Let me be clear: you must have functioning kidneys or dialysis or a transplant to live.
When there’s nothing doing the jobs of the kidneys, there’s no life. Your kidneys filter about 200 quarts of your blood each day. They are the organs that prevent toxic build up in your body by turning these toxins – along with other waste products – into urine. They are responsible for regulating your electrolytes and your blood pressure. These are only three of the many necessary jobs they do.
That would explain why hypertension, also called high blood pressure, is the second leading cause of CKD. Sometimes what is commonly considered medication for hypertension is prescribed for CKD whether or not you have high blood pressure.
The Simple Tests That Could Save Your Life
I’m originally from New York. Do you remember the old lottery advertising slogan from NY, You’ve got to be in it to win it? The same is true here. If you don’t know you have CKD, you won’t be treating it.
You’ll probably feel the needle for the blood test, but that’s a very, very small price to pay for discovering CKD. I have no idea how long I had it before my diagnosis. I could have gone not knowing until I reached end stage which would mean dialysis to perform the jobs my kidneys couldn’t, or a transplant, or… my demise.
The treatment is nothing horrendous. It depends upon your body chemistry (your Comprehensive Metabolic Panel – a blood test – will give you a good picture of that) and your nephrologist’s suggestions. Usually, it’s the hypertension medication mentioned above, a special diet, treating diabetes if you have it, exercise, adequate sleep, and avoiding stress where you can. You can live with that, can’t you? Especially if it means your life.
When I was teaching Essay Writing on the college level, it was a rule never to end your essay with the words, “In conclusion.” But I also taught that you needed to learn the rules, so you could break them.
So… in conclusion, please, please go for the blood and urine tests.
You really don’t need the fatigue, brain fog, or bone problems undiagnosed CKD can cause, much less dialysis or a transplant. Catch the disease early, treat it, and keep living your life!
We would like to thank Gail for contributing this post.
If you would like your story featured on the MyTherapy blog, contact Dan here.
March is National Kidney Month as well as National Women’s Month. Thursday, March 8th was World Kidney Day which was dedicated to women’s kidney health. Mytherapyapp.com asked me if I would guest blog on World Kidney Day. I didn’t hesitate. ANY way to promote awareness of Chronic Kidney Disease is fine with me. The headlines are theirs, but the more I think about them, the more apt I think they are. Thank you, mytherapyapp.com for helping me in my quest to make the world aware of CKD. This is the first part of that guest blog.
The Simple Test That Saved My Life: Gail’s CKD Story
Chronic Kidney Disease is Often Symptomless. When Not Diagnosed, it Can Also Be Deadly
Gail Rae-Garwood
March 8, 2018
This week, chronic kidney disease treatment will cost the US healthcare system almost $1 billion, just as it did last week, and just as it will next week. Treatments such as dialysis and kidney transplants are not only extremely expensive, but a sign that kidney disease has progressed through the stages and become potentially life-threatening. This is usually because it was not detected in the early stages, due to it being a ‘silent disease’ that is often symptomless. Yet, just like another infamously silent disease, hypertension, chronic kidney disease can be diagnosed early with simple tests. When done so, treatment options are usually more simple, cost-effective, and significantly less detrimental to one’s quality of life. Gail Rae-Garwood was fortunate enough to catch chronic kidney disease early. In support of World Kidney Day, Gail has shared her story with us; it highlights how early detection helps save money and, more importantly: lives.
A guest post by Gail Rae-Garwood
My name is Gail Rae-Garwood. I like to think of myself as an average older woman with two adult daughters, a fairly recent husband, and a very protective dog. But I’m not. What makes me a little different is that I have Chronic Kidney Disease… just like the estimated 31 million or 15% of the adult population in the United States. Unlike 96% of those in the early stages of the disease, I know my kidneys are not functioning well.
Chronic Kidney Disease Diagnosis
I was blindsided over a decade ago. That’s when I started seeing a new doctor solely because she was both on my insurance plan and so much closer to home than the one I’d been seeing. It seems everything is at least half an hour away in Arizona; her office wasn’t. As a diligent primary care physician, she ordered a whole battery of tests to verify what she found in my files which, by the way, contained a kidney function reading (called the GFR) of 39%. That was something I’d never been told about.
39%. I’d been a high school teacher for 35 years at that point. If a student had scored 39% on a test, we would have talked and talked until we had gotten to the root of the problem that caused such a low score. No one talked to me about my low kidney function until I changed doctors.
She not only talked, she had me in a nephrologist’s (kidney and hypertension specialist’s) office the next day. That’s when I started worrying. Who gets an appointment with a specialist the very next day? He might have been reassuring, but I’ll never know. I was terrified; he was patriarchal. All I heard was, “I’ll take care of your kidneys. You just do as I say,” or something to that effect.
Nope, wrong doctor for me. I needed to know what was happening, why it was happening, and what I could do about it. I’d already had a terrific Dad and he’d known better than to ask me to give up control of myself.
CKD: What Is It and How Did I Get It?
Nephrologist switch. The new one was much better for me. He explained again and again until I understood and put up with a lot of verbal abuse when this panicky new patient wasn’t getting answers as quickly as she wanted them. Luckily for me, he graciously accepted my apology.
My less-than-stellar experience with being diagnosed and the first nephrologist are what prompted me to write What Is It and How Did I Get It? Early Stage Chronic Kidney Disease. I felt – and still do – that since I taught research writing in college, I should research and then share what I discovered. Why, I wondered, should any new CKD patient be as terrified as I was?
I didn’t feel… well, done with sharing or researching once I finished the book so I began writing a weekly blog: SlowItDownCKD. The blog has won several awards. Basically, that’s because I write in a reader friendly manner. After all, what good is all my researching if no one understands what I’m writing? Non-tech savvy readers asked if I could print the blogs; hence, the birth of the SlowItDownCKD series of books.
What I hit over and over again in the blogs is that diabetes is the foremost cause of CKD with hypertension as the second most common cause. Simple blood and urine tests can uncover your CKD – if you’re part of the unlucky 96% of those in the early stages of the disease who don’t know they have it. That’s important because CKD is mostly symptomless.
Being African-American, Native American or Asian-American
Family history of kidney disease
Abnormal kidney structure
Older age
Older age? Smoking? Obesity? Hypertension? Which was it for me? I have no idea and, frankly, I no longer care. It’s much more important to me that my CKD be treated so I can see my coming grandchild grow up, revel at another daughter’s wedding later this year, and continue to be my sweet husband’s caretaker as well as his wife.
Next week’s blog not only completes this guest blog but contains the most important sentence in it. Cliff hanger? Absolutely! The idea is to get more and more people interested in what CKD is, who may have it, how to detect it, and how to treat it. What better way than a cliff hanger?
Last week I mentioned kidney diet apps and that I suspected the ones I wrote about in SlowItDownCKD 2016 may be outdated or not exist anymore. Let’s jump right in before I need to get up from the computer to walk around for a while. I’ve been working on another book and been sitting here a long time. We all know that’s not good for us.
‘Simply put, an app is a type of software that allows you to perform specific tasks. Applications for desktop or laptop computers are sometimes called desktop applications, while those for mobile devices are called mobile apps.’
During an internet search, I found that NephCure which provides ‘detailed information about the diseases that cause Nephrotic Syndrome (NS) and Focal Segmental Glomerulosclerosis (FSGS)’ (and was one of the first organizations to interview me about CKD, by the way) – at http://nephcure.org/livingwithkidneydisease/managing-your-care/kidney-health-tracking-tools/helpful-mobile-apps/ was way ahead of me in discussing apps. This is what’s on their website:
Diet and Nutrition Apps
• KidneyAPPetite – Gives daily summaries of key nutrients for kidney health, check the nutritional value of foods before you eat it, and provides printable summaries to refer to. Great for patients on a renal diet! Cost: Free, Device: iOS
• Pocket Dietitian – Created by a Nephrologist, allows you to choose your health conditions and dietary restrictions to see recommended foods as well as keep track of what you have eaten. You can even see your past nutrition in graph form. Cost: Free, Device: iOS and Android
• My Food Coach – is designed to help you understand and manage all of your nutritional requirements. This app offers personalized nutrition information, recipes and meal plans. Cost: Free, Device: iOS and Android
• HealthyOut – Enables you to search and order nearby healthy food and browse for healthy options while out to eat. You can even choose a specific diet such as gluten free! Cost: Free, Device: iOS and Android
• Restaurant Nutrition – Allows you to search restaurants and look at nutritional values, locate nearby restaurants, and keep a food journal. The Restaurant Nutrition application shows nutritional information of restaurant foods. Cost: Free, Device: iOS and Android
While I could easily go to most of the apps’ websites by clicking on the name while I held down the control button, this was not the case with Pocket Dietician. I was able to find it and lots of descriptive information about it in the Google Play store, but kept getting the message that I had no devices. The help function on the site was not helpful.
What about My Food Coach? It has an extra feature that my favorite lacked: a warning when a recipe would bring you over your renal diet limits. It’s recipe oriented, which doesn’t endear it to me since I like to experiment cooking my big five ounces of protein daily with my three different size servings of different fruits that are on my renal diet. I also avoid red meat.
HealthyOut, while not specifically for CKD, does have a function for the Mediterranean diet which is more often than not recommended for us. I thought this was a hoot since it never occurred to me that you can check restaurant foods by the restaurant name. I am adding this app to my iPhone.”
It looks like I was wrong. Most of these are still available. Unfortunately KidneyDiet, my all-time favorite, is no more. Neither is Restaurant Nutrition. But let’s see what other apps are available for us.
“Sodium One is a user friendly Sodium Counter app. Patients with High Blood Pressure or Chronic Kidney Disease can benefit from this app a lot. The App allows you to track water intake as well as exercise and weight history. The main focus of Sodium One however, is to manage your daily sodium allowance. The tracking is actually very accurate when it comes to calorie counts. A great extra is that this app does not require an internet connection.”
This is $0.99 and only available in IOS. That’s Apple.
I do want to mention there are apps specifically for those on dialysis. I have not included them in this blog, although NephCure did include KidneyAPPetite. An internet search for ‘dialysis apps,’ or something along that line, will help you find them.
I’ve tried a few other apps that were not dedicated to those with CKD and found moderate success with them. One is Keto, which bills itself as “Stupid Simple”… and it is. However, it’s limited to carbs, fat, and protein. You’re on your own for phosphorous, potassium, and sodium. Oh, KidneyDiet, come back! The nice part of Keto is that you can scan barcodes (Is that really one word these days?) and add your own foods and meals IF you upgrade from the basic free version. Their website at https://play.google.com/store/apps/details?id=com.venninteractive.ssketo tells you this is only available for Android, but I have it on my IOS device.
Under Armour’s MyFitnessPal at https://freepps.top/apps/health-fitness/calorie-counter-myfitnesspal has been around for a while. Again, while this is not perfect for those with CKD, it is a great help. I like that you can set goals and request reminders about your goal, as well as add foods. Of course, Premium offers you a lot more… and charges you accordingly. Articles about exercise and weight pop up, too. And then there are recipes. Again, it doesn’t do the whole trick, although it does count potassium, protein, sodium and calories . What’s missing is phosphorous. The bonuses are carb, fat (by type, no less) cholesterol, fiber, sugar, vitamins A & C, calcium, and iron counters. This is also a free Apple app.
Lose It! at https://www.loseit.com/ is not as comprehensive for the CKD patient. It allows you to track fat, carbs, protein, and calories. Here, again, you can set your goals. You can even take pictures of your food to track it. However, I find I want something more CKD oriented with potassium, phosphorous, and sodium counters included. This looks like it may be a good app for weight loss, but I’m wondering how much help it is for the CKD patient.. This is a free Android app.
At this point, I stopped checking out apps. There are so many more in just a little over the year I last looked at apps. But they’re not quite for the likes of us. It looks like MyFitnessPal is the closest we can come to a kidney app, unless you’re on dialysis. Then I’d go for KidneyAPPetite.
Before I go, here’s a shameless plug for my new book. It’s Sort of Dark Places, available on Amazon and is not CKD related at all. I’ve fictionalized the stories people have told me about their most difficult times. I found it cathartic to write even though these are not my stories. Advance readers have told me they did, too. Give it a try.
In honor of the great Dr. Martin Luther King’s birthday, the first person who hasn’t already won a free book that lets me know they’ve read today’s blog wins a copy of SlowItDownCKD 2012.
A reader asked me how I choose the articles or studies I include in the blogs. Now you’ve got to remember that researching and I go way back. I was fortunate in that Research Writing was my favorite course to teach before I retired as a community college instructor. I loved it.
I was going to give you my take on researching when I stumbled across Dr. Alicia White’s piece on the United Kingdom’s National Health Services site at https://www.nhs.uk/news/Pages/Howtoreadarticlesabouthealthandhealthcare.aspx. She’s already written what I would have, so I’m dedicating today’s blog to that. I have not reproduced all of it only because I don’t have the room in the blog for that. Oh, those are not typos; they’re the UK spelling. Take it away, Dr. White:
If you’ve just read a health-related headline that has caused you to spit out your morning coffee (“Coffee causes cancer” usually does the trick), it’s always best to follow the Blitz slogan: “Keep Calm and Carry On”. On reading further, you’ll often find the headline has left out something important, such as: “Injecting five rats with really highly concentrated coffee solution caused some changes in cells that might lead to tumours eventually (study funded by The Association of Tea Marketing).”
The most important rule to remember is: don’t automatically believe the headline. …, you need to analyse the article to see what it says about the research it is reporting on….
Does the article support its claims with scientific research?
Your first concern should be the research behind the news article. If an article touts a treatment or some aspect of your lifestyle that is supposed to prevent or cause a disease, but doesn’t give any information about the scientific research behind it, then treat it with a lot of caution. The same applies to research that has yet to be published.
Is the article based on a conference abstract?
Another area for caution is if the news article is based on a conference abstract. Research presented at conferences is often at a preliminary stage and usually hasn’t been scrutinised by experts in the field. Also, conference abstracts rarely provide full details about methods, making it difficult to judge how well the research was conducted. …
Was the research in humans?
Quite often, the “miracle cure” in the headline turns out to have only been tested on cells in the laboratory or on animals. … Studies in cells and animals are crucial first steps and should not be undervalued. However, many drugs that show promising results in cells in laboratories don’t work in animals, and many drugs that show promising results in animals don’t work in humans. If you read a headline about a drug or food “curing” rats, there is a chance it might cure humans in the future, but unfortunately a larger chance that it won’t…..
How many people did the research study include?
In general, the larger a study the more you can trust its results. Small studies may miss important differences because they lack statistical “power”, and are also more susceptible to finding things (including things that are wrong) purely by chance. … When it comes to sample sizes, bigger is usually better. So when you see a study conducted in a handful of people, treat it with caution.
Did the study have a control group?
…. If the question being asked is about whether a treatment or exposure has an effect or not, then the study needs to have a control group. A control group allows the researchers to compare what happens to people who have the treatment/exposure with what happens to people who don’t. …
Also, it’s important that the control group is as similar to the treated/exposed group as possible. The best way to achieve this is to randomly assign some people to be in the treated/exposed group and some people to be in the control group. This is what happens in a randomised controlled trial (RCT) and is why RCTs are considered the “gold standard” for testing the effects of treatments and exposures. … Without either, retain some healthy scepticism.
Did the study actually assess what’s in the headline?
…. For example, you might read a headline that claims: “Tomatoes reduce the risk of heart attacks.” What you need to look for is evidence that the study actually looked at heart attacks. You might instead see that the study found that tomatoes reduce blood pressure. This means that someone has extrapolated that tomatoes must also have some impact on heart attacks, as high blood pressure is a risk factor for heart attacks. Sometimes these extrapolations will prove to be true, but other times they won’t. Therefore if a news story is focusing on a health outcome that was not examined by the research, treat it with a pinch of salt.
Who paid for and conducted the study?
This is a somewhat cynical point, but one that’s worth making. The majority of trials today are funded by manufacturers of the product being tested – be it a drug, vitamin cream or foodstuff. This means they have a vested interest in the results of the trial, which can potentially affect what the researchers find and report in all sorts of conscious and unconscious ways. This is not to say that all manufacturer-sponsored trials are unreliable. Many are very good. However, it’s worth seeing who funded the study to sniff out a potential conflict of interest….
Many thanks to Dr. White for her explanations.
Here we are in the middle of madness, holiday madness that is. Of course, that means we need to remind ourselves to slow down and de-stress. Exercising is one way to de-stress. We all have different ways to do that. The important thing is to do it… and stick to your renal diet if you follow one.
To those of who you celebrate Chanukah, I wish you a happy and a healthy first night tomorrow night. We’ll be lighting the Menorah along with you. It’ll be hard not to eat the chocolate gelt (money), but you can do it.
Considering my family’s history, I’m vigilant about having colonoscopies. This year, however, there was an additional test – an endoscopy. You may have heard of this as an upper endoscopy, EGD or esophagogastroduodenoscopy. The names are interchangeable. Whatever you call it, I was intrigued.
An upper endoscopy is used to diagnose and, sometimes, treat conditions that affect the upper part of your digestive system, including the esophagus, stomach and beginning of the small intestine (duodenum).
Upper GI endoscopy is a procedure in which a doctor uses an endoscope—a flexible tube with a camera—to see the lining of your upper GI tract. A gastroenterologist, surgeon, or other trained health care professional performs the procedure, most often while you receive light sedation to help you relax.
Relax? I was out like a light. First I was being shown was the device that was going to hold my mouth open and hold the tube that would be going down my throat, the next second I awoke in my room… or so it seemed.
A gastroscopy may be advised if you have symptoms such as:
• Repeated (recurring) indigestion.
• Recurring heartburn.
• Pains in the upper tummy (abdomen).
• Repeatedly being sick (vomiting).
• Difficulty swallowing.
• Other symptoms thought to be coming from the upper gut.
The sort of conditions which can be confirmed (or ruled out) include:
• Inflammation of the gullet (oesophagus), called oesophagitis. The operator will see areas of redness on the lining of the oesophagus.
• Stomach and duodenal ulcers. An ulcer looks like a small, red crater on the inside lining of the stomach or on the first part of the gut (small intestine) known as the duodenum.
• Inflammation of the duodenum (duodenitis) and inflammation of the stomach (gastritis).
• Stomach and oesophageal cancer.
• Various other rare conditions.
“CKD adversely affects digestive function,” the authors write. “Abnormalities in digestive secretion and absorption may potentially have a broad impact in the prevention and treatment of both CKD and its complications.”
Not good. We know that CKD requires close monitoring and life style changes. This may be another facet of the disease to which we need to pay attention.
I had some biopsies while I was under sedation. Nope, didn’t feel a thing.
But I now know I have gastritis and an irregular Z-line. The silver lining here is that I don’t have Helicobacter pylori or H. pylori, a type of bacteria that infects the stomach which can be caused by chronic gastritis. Mine seems to be the food caused kind. Generally it’s alcohol or caffeine, spicy foods, chocolate, or high fat foods that can cause this problem. I don’t drink, eat spicy or high fat foods, and rarely eat chocolate, but nooooooooooooooooo, please don’t take away those two luscious cups of coffee a day.
I wasn’t sure what this Z-line thing was so started poking around on the internet, since I didn’t catch it before seeing the gastroenterologist for my after visit appointment. Dr. Sidney Vinson, University of Arkansas for Medical Sciences/UAMS College of Medicine explained:
This refers to the appearance of the tissue where the esophagus and stomach meet. The z-line is a zig-zag line where these 2 different type tissues meet. Occasionally it can be irregular and protrude more into the esophagus and not have the typical appearance. This is generally a benign condition but can occasionally represent mild barrett’s esophagus, a precancerous change caused by reflux.
Apparently my normal duodenum was biopsied to see if my doctor could find a reason for the pain I was experiencing in the upper stomach. Well, it was more discomfort than pain, but he wanted to be certain there wasn’t an ulcer… and there were no ulcers. Yay!
Hmmm, I have gastritis which is an inflammation and CKD, which is an inflammatory disease. Which came first? Did it matter? If I treat one will the other improve? I’ve been following the renal diet for all nine years since my diagnose and have made the appropriate life style changes, too.
What more could I do? There’s the ever present to struggle to lose weight. That could help. I wasn’t willing to take more medication as my gastroenterologist understood and accepted. I was already taking probiotics. I examined the little booklet produced by Patient Point that I was given more closely ignoring all the advertisements for medication.
Look at that. It seems sleeping on your left side can help. “Since your stomach curves to your left, part of it will be lower than your esophagus.” I can do that, although I wonder if it will be awkward while wearing the BiPap.
I also learned that skipping late night snacks and eating smaller meals would be helpful since there would be less acid produced by smaller meals and I wouldn’t have to deal with acid while I slept if I stopped eating at least two hours before bedtime. Acid is produced to help digest your food.
For Thanksgiving, I was part of a video produced by Antidote Me (the clinical trial matching program I wrote about several weeks ago). The topic was What I Am Thankful to Medical Research for. I think I can safely add endoscopy to that list. https://drive.google.com/file/d/1Mwv-vBRgzRFe8-Mg6Rs7uUIXMOgOMJHX/view
I was also invited to participate in two separate book signings and have a video from one of them. I’ll post it as soon as I can figure out how since I don’t own the rights yet. Oh, I feel a new year’s resolution coming on – learn more about the technology I need for my writing.
I know, I know. When you see that question on an application, you want to answer ‘yes,’ but you’re only given the choice of male or female. Well, at least that’s my experience. Okay, got that out of the way.
I haven’t found too much about sex that’s different from the problems of non-CKD patients although with this disease there may be a lower sex drive accompanied by a loss of libido and an inability to ejaculate. Usually, these problems start with an inability to keep an erection as long as usual. The resulting impotency has a valid physical, psychological or psycho-physical cause.
Some of the physical causes of impotence, more recently referred to as Erectile Dysfunction [E.D.] for a CKD patient could be poor blood supply since there are narrowed blood vessels all over the body. Or maybe it’s leaky blood vessels. Of course, it could be a hormonal disturbance since the testicles may be producing less testosterone and the kidneys are in charge of hormones….
While E.D. can be caused by renal disease, it can also be caused by diabetes and hypertension. All three are of importance to CKD patients. Sometimes, E.D. is caused by the medications for hypertension, depression and anxiety. But, E.D. can also be caused by other diseases, injuries, surgeries, prostate cancer or a host of other conditions and bodily malfunctions. Psychologically, the problem may be caused by stress, low self-esteem, even guilt to name just a few of the possible causes….
Women with CKD may also suffer from sexual problems, but the causes can be complicated. As with men, renal disease, diabetes and hypertension may contribute to the problem. But so can poor body image, low self-esteem, depression, stress and sexual abuse. Any chronic disease can make a man or a woman feel less sexual….
Common sense tells us that sex or intimacy is not high on your list of priorities when you’ve just been recently diagnosed….
Sometimes people with chronic diseases can be so busy being the patient that they forget their partners have needs, too. And sometimes, remembering to stay close, really close as in hugging and snuggling, can be helpful….
It’s important to remember that people with kidney failure can have healthy marriages and meaningful relationships. They can fall in love, care for families, and be sexual. Staying intimate with those you love is important. It’s something everyone needs.
Many people think that sexuality refers only to sexual intercourse. But sexuality includes many things, like touching, hugging, or kissing. It includes how you feel about yourself, how well you communicate, and how willing you are to be close to someone else.
There are many things that can affect your sexuality if you have kidney disease or kidney failure — hormones, nerves, energy levels, even medicine. But there are also things you and your healthcare team can do to deal with these changes. Don’t be afraid to ask questions or get help from a healthcare professional.
Once again, it’s important to remember, you are not alone.
There are no limits with regard to sexual activities you may engage in as a patient with renal disease, as long as activity does not place pressure or tension on the access site, causing damage. (Me: This is for advanced CKD.)
If you are sexually active, practicing safe sex and/or using birth control are needed, even if you think you may be physically unable to have children.
Activities such as touching, hugging and kissing provide feelings of warmth and closeness even if intercourse is not involved. Professional sex therapists can recommend alternative methods as well.
Keeping an open mind and having a positive attitude about yourself and your sexuality may lower the chances of having sexual problems.
There are both medical and emotional causes for sexual dysfunction. The reason for your dysfunction can be determined through a thorough physical exam in addition to an assessment of your emotional welfare and coping skills.
Relaxation techniques, physical exercise, writing in a journal and talking to your social worker or a therapist can help you to feel better about your body image and/or sexual dysfunction.
Resuming previous activities, such as dining out or traveling, as a couple or single adult, can be helpful.
Provide tokens of affection or simple acts of kindness to show you care.
Communicate with your partner or others about how you feel.
Fatigue is a major factor. Any chronic illness is tiring, and chronic kidney disease, which is often accompanied by anemia and a demanding treatment, practically guarantees fatigue.
Depression is another common issue. Almost everyone experiences periods of depression, and one of the symptoms of depression is loss of interest in sexual intimacy.
Medications can also affect one’s ability or desire to have intercourse. Since there may be other medications which are just as effective without the side effect of loss of sexual function or desire, talk to your doctor about your pills.
Feelings about body image Having a peritoneal catheter, or a fistula or graft, may cause some people to avoid physical contact for fear of feeling less attractive or worrying about what people think when they look at them. (Me: Again, this is for late stage CKD.)
Some diseases, such as vascular disease and diabetes, can lead to decreased blood flow in the genital area, decreased sexual desire, vaginal dryness and impotence.
It looks like the information about CKD and sexuality hasn’t changed that much, but it does seem to be more available these days.
Every once in a great while, I’ll come across a Chronic Kidney Disease book that I want to share. I think there were only three or four of these in the last six years. Today, I add another one. Dr. Kang, the author, is a local doctor. That was the first thing that caught my eye.
I thought I would be reading the usual information … and I did, but it was written with verve and included some information I hadn’t known. So I did the obvious. I contacted the good doctor to see if he’d be interested in sharing his knowledge with us on the blog. I’m so very glad he agreed.
Dr. Mandip S.Kang, is not only a senior partner in Southwest Kidney Institute right here in Phoenix, but he is also a Fellow in the American Society of Nephrologists I like so much. Just last week, I gleefully accepted their invitation to join the Twitter chat (#AskASN) about staging in CKD and often refer to them in both my blogs and books. He is also the author of the IBPA Gold Award winning book: The Doctor’s Kidney Diets……A Nutritional Guide to Managing and Slowing The Progression of Chronic Kidney Disease, the book that caught my eye.
This is what he wrote for us:
Receiving a diagnosis of kidney disease is not a death sentence for patients, but is often overwhelming and a life changing event. Patients are often confused and the information they receive from different healthcare providers may not be the same. Patients often ask, “What should I do?”
Having experience as a former Assistant Clinical Professor of Medicine at University of Utah School of Medicine and currently as a Senior Nephrologist (kidney specialist), I have gained some insight into how to alleviate my patients’ fears and I have come up with a four point plan that I try to teach my kidney patients. I believe that the role of the physician is to be a teacher and a coach as patients navigate their way into the complexities of a Chronic Kidney Disease diagnosis. I believe that every kidney specialist should have a chalk board in the patient exam rooms and lay out the plan for his or her approach to their patients just like we were taught in schools.
Here is a four point plan that all kidney patients should remember as they visit their kidney specialists and at home. The acronym for the plan is very simple: D.A.M.E.
1. ‘D’ in the acronym stands for diet. The reason I chose diet first comes from the Chinese wisdom in treating any disease: ‘He that takes medicine and neglects diet, wastes the skills of the physician.’ Patients must be taught what the kidney diet is and why they need to follow it for the rest of their lives. Since the kidney diet is complex, they must be provided with educational materials that outline the diet and be strongly encouraged to visit a kidney dietitian who will tell them what and how much to eat.
Dietitians and kidney doctors will teach them about the benefits of eating fresh foods and avoiding processed foods. Patients should remember that the ‘p’ in ‘p’rocessed foods is akin to ‘p’acked with calories. Learning to read a Nutrition Facts label is a must if the doctor wants to do all he or she can to help the patient slow down – and sometimes halt – the progression of kidney disease. It is important to remember that in the earlier stages of kidney disease, the diet may not be as strict – but if progression of the disease is noted, then dietary modifications are more stringent and frequent laboratory tests may need to be performed to assess progress.
2. ‘A’ in the four point CKD plan stands for activity. “What is activity?” you might say. It could mean walking more, taking more steps daily, joining a gym, hiking, biking or any activity that keeps you on your feet. As most Americans already know, the obesity rates in the USA are skyrocketing leading to most chronic health conditions such as Chronic Kidney Disease, Coronary Artery Disease, Stroke, Arthritis, Lung Disease, etc. These chronic health conditions stem from lack of activity and consuming excessive calories. Many patients lead a sedentary lifestyle such as watching TV for long hours which leads to worsening of their health issues. Patients should be encouraged to do the activities they enjoy the most such as dancing, or walking in a park or on a beach. Patients should weigh themselves on a weekly basis to monitor their weight.
3. ‘M’ in the acronym stands for medications that your doctor prescribes. Your doctor may also tell you not to take certain over the counter medications that may harm your kidneys such as Advil, Motrin, Aleve, Ibuprofen, Celebrex, Prilosec, herbal remedies, etc. I encourage all patients to memorize their medications and keep a list with them at all times. Remember that all medications are prescribed because the benefit to the patient outweighs the risk and no medication is entirely safe; therefore, it should be taken as prescribed and any side effects reported to your doctor. You should not take any new medicine unless it has been cleared by your kidney specialist.
4. ‘E’ in the above acronym stands for education. This is the key element in the D.A.M.E plan to treat patients with CKD. Unless the patient has a clear understanding of their disease process, labs, treatment plan, and the role of diet, activity, and medications, they will not be successful in managing and slowing the progression of Chronic Kidney Disease. How well a patient does will depend on their knowledge of their disease and if they comply with the instructions given to them by the kidney doctors.
I hope that all kidney doctors and patients keep the D.A.M.E. acronym in mind. Patients who are active participants in their care lead healthier and productive lives. I wish all of the readers well.
I hadn’t heard of the D.A.M.E. method before but I like it, especially “the ‘p’ in ‘p’rocessed foods is akin to ‘p’acked with calories.” Many thanks, Dr. Kang, for introducing this common sense theme to us.
Here’s hoping everyone had a wonderful Father’s Day. During our relaxed celebration for Bear, I found myself ruminating about how many times we’ve celebrated this holiday for fathers no longer with us and how many more times we would be able to celebrate it for the fathers who are. They are aging. Wait a minute, that means their kidneys are aging, too.
Yep, that meant a new blog topic. We already know that kidney function declines with age. According to the National Kidney Foundation at https://www.kidney.org/blog/ask-doctor/what-age-do-kidneys-decline-function, “The general ‘Rule of Thumb’ is that kidney function begins to decline at age 40 and declines at a rate of about 1% per year beyond age forty. Rates may differ in different individuals.” 40?
Well, what is a perfect kidney function score… if such exists? Back to the NKF, although they call this a ‘normal’ not ‘perfect’ GFR, this time at https://www.kidney.org/atoz/content/gfr:
In adults, the normal GFR number is more than 90. GFR declines with age, even in people without kidney disease.
Average estimated GFR
20–29 116
30–39 107
40–49 99
50–59 93
60–69 85
70+ 75
Got it. So even for a normal 70+ person, I have CKD with my 50ish GFR.
“Glomerular filtration rate [if there is a lower case “e” before the term, it means estimated glomerular filtration rate] which determines both the stage of kidney disease and how well the kidneys are functioning.”
No, that won’t do. I think we need more of an explanation. This is from SlowItDownCKD 2015:
“Glomerular filtration rate (GFR) is a test used to check how well the kidneys are working. Specifically, it estimates how much blood passes through the glomeruli each minute. Glomeruli are the tiny filters in the kidneys that filter waste from the blood.
Okay, I think that’s clear now. However, that’s not what I wanted to know. This is – if kidney function already declines with age, does having CKD age us more quickly?
“Premature aging is a process associated with a progressive accumulation of deleterious changes over time, an impairment of physiologic functions, and an increase in the risk of disease and death. Regardless of genetic background, aging can be accelerated by the lifestyle choices and environmental conditions to which our genes are exposed. Chronic kidney disease is a common condition that promotes cellular senescence and premature aging through toxic alterations in the internal milieu. This occurs through several mechanisms, including DNA and mitochondria damage, increased reactive oxygen species generation, persistent inflammation, stem cell exhaustion, phosphate toxicity, decreased klotho expression, and telomere attrition….”
“Chronic kidney disease (CKD) shares many phenotypic similarities with other chronic diseases, including heart failure, chronic obstructive pulmonary disease, HIV infection and rheumatoid arthritis. The most apparent similarity is premature ageing, involving accelerated vascular disease and muscle wasting. We propose that in addition to a sedentary lifestyle and psychosocial and socioeconomic determinants, four major disease-induced mechanisms underlie premature ageing in CKD: an increase in allostatic load, activation of the ‘stress resistance response’, activation of age-promoting mechanisms and impairment of anti-ageing pathways. The most effective current interventions to modulate premature ageing—treatment of the underlying disease, optimal nutrition, correction of the internal environment and exercise training—reduce systemic inflammation and oxidative stress and induce muscle anabolism. Deeper mechanistic insight into the phenomena of premature ageing as well as early diagnosis of CKD might improve the application and efficacy of these interventions and provide novel leads to combat muscle wasting and vascular impairment in chronic diseases.”
Remember the friend of my daughter’s who hadn’t seen me in five years who (thought) he whispered to her, “Your mom got so old.” Now I understand why, although I have noticed this myself. I look in the mirror and see the bags under my eyes that are not errant eye liner. I see the lines in my faces, especially around my mouth, that weren’t there just a year ago. I see the stubborn fat around my middle that frustrates me no end. I see that it takes me forever (okay, so I’m being figurative here, folks) to recover from the flu, and I see how easily I become – and stay – tired. The dancer in me screams, “No fair!” The adult patient in me says, “Deal with it,” so I do.
I’ve used quite a bit of advanced terminology today, but haven’t explained a great deal of it in the hopes that when you read these articles their meanings will become clear in context. If they don’t, please leave me a comment and I will explore each one of them in future blogs. Who knows? Maybe I’ll need to devote an entire blog to whichever term it is you’d like to know more about.
Don’t let our premature aging get you down. We can work against it and, hopefully, slow it down just as we do with the progress of the decline in our kidney function.
I have been saving this bit of news for the last item in today’s blog. The world is not going to suffer if it doesn’t know about my photography, my teaching ,writing, or acting careers. But, when it comes to CKD, my writing can add something for those 31 million people who have it…especially the 90% that haven’t been diagnosed yet. What I did was completely change my web site so that it deals only with my Chronic Kidney Disease Awareness Advocacy (It’s all caps because that’s the way I think of it.) under the umbrella of SlowItDownCKD. I have to admit, I was surprised to see how active I’ve been in the last decade. It’s different when you see your work listed all in one place. Take a look at www.gail-raegarwood.com and tell me what you think, would you?
I was in Cuba last week with very sketchy internet, so it was not possible to post a blog. But for now, I was thinking about a friend – you know, one of those Facebook friends you never met but you feel an instant kinship with – who told me that her surgeon warned her that her recovery from the spinal fusion surgery she’d recently had would be slow because she has Chronic Kidney Disease.
CKD…bone healing. Let’s start slowly and work this one out. First of all, what do the kidneys have to do with your bones?
“Both vitamin D and calcium are needed for strong bones. It is yet another job of your kidneys to keep your bones strong and healthy….Vitamin D enables the calcium from the food you eat to be absorbed in the body. CKD may leech the calcium from your bones and body….Be aware that kidney disease can cause excessive phosphorus. And what does that mean for Early Stage CKD patients? Not much if the phosphorous levels are kept low. Later, at Stages 4 and 5, bone problems including pain and breakage may be endured since excess phosphorous means the body tries to maintain balance by using the calcium that should be going to the bones.”
Whoa! Each one of those thoughts needs at least a bit more explanation. Let’s start with the jobs of the kidneys. The Book of Blogs: Moderate Stage Chronic Kidney Disease, Part 1has a paragraph that mentions some of them. I turned it into a list to make it more visual.
“Our kidneys are very busy organs, indeed. They produce urine, remove potentially harmful waste products from the blood, aid in the maintenance of the local environment around the cells of the body,
help to stimulate the production of red blood cells, regulate blood pressure, help regulate various substances in the blood {For example, potassium, sodium, calcium and more}, help to regulate the acidity of the blood, and regulate the amount of water in the body. Mind you, these are just their main jobs.”
Another of those various substances in the blood they help to regulate is phosphorous. That’s where one of the connections between CKD and your bones lies. If your phosphorous is not being correctly regulated by your kidneys (since your kidneys are impaired), yes you do experience pain and broken bones, but did you notice that your body also diverts your necessary-for-bone-health calcium to regulate the other substances in your blood?
“This is the second most plentiful mineral in the body and works closely with the first, calcium. Together, they produce strong bones and teeth. 85% of the phosphorous and calcium in our bodies is stored in the bones and teeth. The rest circulates in the blood except for about 5% that is in cells and tissues…. Phosphorous balances and metabolizes other vitamins and minerals including vitamin D which is so important to CKD patients. As usual, it performs other functions, such as getting oxygen to tissues and changing protein, fat and carbohydrate into energy.”
“When your kidney function declines, you are unable to get rid of excess phosphate. (Me here: that’s what we call phosphorous except when dealing with inorganic chemistry.) The phosphate builds up in your body and binds to calcium, which, in turn, lowers your calcium levels. When your calcium levels get too low, glands in your neck (called the parathyroid glands) pull the extra calcium your body needs out of your bones. This can make your bones easy to break. The bound phosphate and calcium get deposited in your blood vessels. It can increase your risk of heart disease and stroke. It can also cause skin ulcers and lumps in your joints.”
So where does vitamin D come in? As was mentioned in SlowItDownCKD 2015,
“’Vitamin D: Regulates calcium and phosphorous blood levels as well as promoting bone formation, among other tasks – affects the immune system.’ We know vitamin D can be a real problem for us. How many of you are taking vitamin D supplements? Notice my hand is raised, too. How many of you read the blogs about vitamin D? Good!”
But, you know, it’s never just that easy. As CKD patients, we have limits of how much protein, potassium, sodium, and – wait for it – phosphorous we can eat each day. There is no socking in all the good stuff for kidney disease patients.
I can see why my friend’s surgeon told her the recovery might be slow. Something else that keeps the bones strong is weight bearing exercise, but how can she do that right now?
Remember when I was lucky enough to catch the flu just after Christmas? (She wrote sarcastically.) When I went to the Immediate Care facility my doctor is associated with, the doctor there had my records and knew I’d had pleurisy at one time. But now, he ordered a chest x-ray to check for pneumonia. What he found instead was news to me… so, of course, I’m telling you about it.
“What? The what? Oh, the thorax. That’s ‘the part of the human body between the neck and the diaphragm, partially encased by the ribs and containing the heart and lungs; the chest’ according to The Free Dictionary at http://www.thefreedictionary.com/thorax.”
Thoracic is the adjective form of thorax; it describes the aorta in this case.
“The aorta gives off branches that go to the head and neck, the arms, the major organs in the chest and abdomen, and the legs. It serves to supply them all with oxygenated blood. The aorta is the central conduit from the heart to the body.”
Now I get the connection between Chronic Kidney Disease and the aorta. Did you catch “oxygenated blood” in that definition? And what organs oxygenate the blood? Right. Your kidneys. This excerpt from SlowItDownCKD 2015 may help.
““The National Kidney and Urologic Diseases Information Clearinghouse …explains.
‘Healthy kidneys produce a hormone called erythropoietin, or EPO, which stimulates the bone marrow to produce the proper number of red blood cells needed to carry oxygen to vital organs. Diseased kidneys, however, often don’t make enough EPO. As a result, the bone marrow makes fewer red blood cells.’”
With me so far? Now, what the heck is an unfolded aorta? I turned to the British site for radiologists, Radiopaedia.org, at https://radiopaedia.org/articles/unfolded-aorta for the definition. “The term unfolded aorta refers to the widened and ‘opened up’ appearance of the aortic arch on a frontal chest radiograph. It is one of the more common causes for apparent mediastinal widening and is seen with increasing age.
It occurs due to the discrepancy in the growth of the ascending aorta with age, where the length of the ascending aorta increases out of proportion with diameter, causing the plane of the arch to swivel.”
I purposely left the click through definitions in so you read them for yourself. You know the drill: click on the link while holding down your control key. For those of you who are reading the print version of the blog, just add the definition of aorta to the common terms we know: arch and ascending.
Mediastinal, according to the Merriam-Webster Dictionary at https://www.merriam-webster.com/dictionary/mediastinum is the adjective (describing) form of mediastinum or “the space in the chest between the pleural sacs of the lungs that contains all the tissues and organs of the chest except the lungs and pleurae; also: this space with its contents.”
“The pleura refers to the 2 membranes that cover the lungs and line the chest cavity. The purpose of the pleura is to cushion the lungs during respiration.
Side note: I definitely feel like I’m back teaching a college class again.
Okay, so now we have a bunch of definitions, we’ve put them together as best we can and where does it bring us? Are you ready for this? Nowhere. An unfolding of the thoracic aorta is nothing more than a function of age.
However, with CKD, it’s somewhere. As was explained in What Is It and How Did I Get It? Early Stage Chronic Kidney Disease, “Hemoglobin is the protein in red blood cells that carries oxygen from the lungs to the rest of the body.” We’re already not getting enough oxygen due to our poor, declining in function kidneys.
Am I concerned about the unfolding thoracic aorta? No, not at all. It happens with age; I don’t think I can do anything about that. But, the CKD that also lowers our oxygen production? Oh yes, I can – do – and will do something about that by protecting my kidneys as best I can and keeping the remaining kidney function I have.
“Along with taking your prescribed blood pressure medications, lifestyle changes such as losing weight, exercising, meditating, eating less sodium, drinking less alcohol and quitting smoking can help lower blood pressure. Better blood pressure control helps preserve kidney function.”
I added using my sleep apnea machine and aiming for eight hours of sleep a night. I also stick to my renal diet – which limits protein, phosphorous, potassium, and sodium (as mentioned by kidney.com) – for the most part and keeping my kidneys hydrated by drinking at least 64 ounces of fluid a day.
Is it hard? I don’t know any more. It’s been nine years. They’re simply habits I’ve developed to live as long as I can and, sometimes, even raise the function of my kidneys.
When my New York daughter was with us over the holidays, I realized how differently we eat than other people do. My husband has chosen to pretty much eat the way I do. So she actually had to go down to the market to pick up the foods that people ordinarily eat. It would have been funny if I hadn’t been sick. I would have gone with her and laughed each time I answered, “No,” when she asked, “Do you eat this?”
Today is Martin Luther King’s birthday. Today, more than ever, we need to heed his message. Whether you apply it to today’s bizarre political scene, your local community, your family, your co-workers doesn’t matter. What matters is the operant word: doing.
That picture and those words got me to thinking. What AM I doing for others? And what still needs to be done?
My commitment is to spread awareness of Chronic Kidney Disease (CKD). As a patient myself, I know how important this is. As you know, CKD is a costly, lethal disease if not caught early and treated… and it’s not just older folks – like me – who are at risk. One out of ten people worldwide has CKD, yet an overwhelming number of them are unaware they have it.
We also know the disease can be treated, just not the way you’d usually expect a disease to be treated. A diet with restrictions on protein, potassium, phosphorous and sodium is one aspect of that treatment. Exercise, adequate sleep, and avoiding stress are some of the other aspects. Some patients – like me – may have to take medication for their high blood pressure since that also affects kidney function. Imagine preventing a death with lifestyle changes. Now image saving the lives of all those who don’t know they have CKD by making them aware this disease exists. Powerful, isn’t it?
We’re all aware by now that the basic method of diagnosing CKD is via routine blood and urine tests. Yet, many people do not undergo these tests during doctor or clinic visits, so don’t know they have Chronic Kidney Disease, much less start treating it. That’s where I come in; I tell people what can be done. I tell people how they can be diagnosed and treated, if necessary.
Healthline is a well-respected, informative site for medical information. This past year this blog, SlowItDownCKD, was a winner in their list of The Six Best Kidney Disease Blogs. That brought the hits on my page up by the hundreds. That means hundreds more people are now aware of Chronic Kidney Disease, how it is diagnosed, how it is treated, and how to live with it.
But not everything is working as I’d hoped it would. Unfortunately, I am still not having success in having Public Service Announcements placed on television or radio. Nor have I been able to interest most general magazines or newspapers in bringing the disease to the public’s awareness.
It hasn’t totally been a wipeout there, though. Michael Garcia did interview me onThe Edge Podcast and both Nutrition Action Healthletter, Center for Science in the Public Interest (the nation’s largest-circulation nutrition newsletter) and New York State United Teachers (membership 600,000) ‘It’s What We Do’ profiled my work spreading CKD Awareness. Profiling my work, interviewing me, mentioning the blog all bring awareness of Chronic Kidney Disease to the public. Awareness leads to testing. Testing leads to diagnosing. Diagnosing leads to treatment. Treatment leads to saving lives. This is why I do what I can to spread awareness of Chronic Kidney Disease.
What about you? Can you speak about CKD with your family? Your friends? Your co-workers? Your brothers and sisters in whichever religion you follow? What about your neighbors? I was surprised and delighted at the number of non CKD friends and neighbors who follow the blog. When I asked why they did, they responded, “I have a friend….” We may all have a friend who may have CKD, whether that friend has told us yet or not.
There are more formal methods of spreading this awareness if that interests you. The National Kidney Foundation has an Advocacy Network.
“A NKF Advocate is someone who has been affected by kidney disease, donation or transplant and who wants to empower and educate others. These include people with kidney disease, dialysis patients, transplant recipients, living donors, donor family members, caregivers, friends and family members.
Advocacy plays an integral role in our mission. You can make a significant difference in the lives of kidney patients by representing the National Kidney Foundation. We give you the tools you need to make your voice heard.”
The American Kidney Fund also has an advocacy program, but it’s a bit different.
“There is strength in numbers. More than 5,100 passionate patients, friends, loved ones and kidney care professionals in our Advocacy Network are making a huge difference on Capitol Hill and in their own communities. Together, we are fighting for policies that improve care for patients, protect patients’ access to health insurance and increase funding for kidney research. As advocates, we play a key role in educating elected officials and our communities about the impact of kidney disease.”
Obviously, I’m serious about doing that which will spread awareness of CKD. You can take a gander at my website, www.gail-raegarwood.com, to see if that sparks any ideas for you as to how you can start doing something about spreading awareness of CKD, too. I urge you to do whatever you can, wherever you can, and whenever you can.
Happy New Year and welcome to 2017. We did our usual stay in, watch movies, and toast with non-alcoholic champagne (I know that’s contradictory.) at midnight. With our New York daughter here, it was even more meaningful.
A new year brings to mind new beginnings… and that leads me to Part 3 of the miracle series, as promised. I am so, so serious about this and hope you decide to take on for yourself causing a miracle in CKD by sharing information.
I was thinking about social media the other day. Where are the public service announcements about Chronic Kidney Disease? I am still – nine years after my diagnose – knocking on seemingly closed doors to encourage Public Service Announcements everywhere. While the public doesn’t seem as involved with network television or radio as they were when I was younger, we now have Twitter, Facebook, Instagram, LinkedIn, and Tumblr to name just a few ways we can share.
I use a both a Facebook page and a Twitter account to post one fact about or information pertinent to those with CKD daily. Join me at SlowItDownCKD on Facebook and @SlowItDownCKD on Twitter. I also monitored Libre’s Tweet Chat with Gail Rae 1/10/12. I knew nothing about Twitter at the time, but it was a way to share the information I had. You may not want to do this, but feel free to ‘steal’ the information posted and share it with others.
There are also Podcasts, Internet Radio Shows, YouTubes, etc. to share what the public needs to know about CKD. A YouTube can be viewed by one person who posts it on Facebook and go viral. Don’t bother looking at mine. They’re pretty painful. I’ll look into this again at a later date.
On the other hand, these are some of the social media venues that interviewed me: The Edge
Podcast 5/9/16, Online with Andrea 3/23/15 & 3/07/12, What Is It? How Did I Get It? 2/17/12, and Improve Your Kidney Health with Dr. Rich Snyder, DO 11/21/11. I never knew these venues existed before I started working towards the miracle I wanted to cause.
Lo and behold, my sharing brought others who wanted to know about CKD, so I was profiled by Nutrition Action Healthletter, Center for Science in the Public Interest 9/16, New York State United Teachers ‘It’s What We Do’ 8/9/16, and Wall Street Journal ‘Health Matters’ 1/13/14. Remember that Clairol commercial in last week’s blog?
Let’s say you agree that sharing can cause a miracle in Chronic Kidney Disease and want to join in living a life causing this miracle. The first thing you’d want to do is learn about CKD. The American Kidney Fund and the National Kidney Foundation both have a wealth of information written for the lay person, not the medical community. By the way, the National Kidney Foundation also has information about CKD globally. Maybe you’d rather join in World Kidney Day gatherings and distribute materials. Then keep an eye on World Kidney Day’s Twitter account for locations around the world.
As you can see, I’ve been creating this miracle is by writing for these organizations and more kidney specific ones, as well as guest blogging for various groups. You may not choose to do that… but you can speak at your religious group meetings, your sports league, your weekly card game, or whatever other group you’re comfortable with.
A miracle doesn’t have to be profound. You can help create this one. All you need is a little education about CKD and the willingness to introduce the subject where you haven’t before.
I live my life expecting miracles and I find they happen. This miracle that I’m causing – and is happening – has been (and is) created by sharing, sharing, sharing. The more than 200 million people who have Chronic Kidney Disease need this information, to say nothing of those who have yet to be diagnosed.
There aren’t that many organs to go around for those who didn’t know they had CKD and progressed to End Stage Renal Disease. We know that transplantation is a treatment, not a cure, and one that doesn’t always last forever. We also know that kidneys from living donors usually last longer than those from cadaver donors. Share that, too.
We have our no cost, no pain, no tools needed miracle right on our lips… or at our fingertips. Start sharing, keep sharing, urge others to share, and help to prevent or slow down the progression in the decline of kidneys worldwide. Sharing is causing a miracle in CKD. Both deaths and hospitalizations for this disease have declined since 2008. If that isn’t a miracle, I don’t know what is. I keep saying I live my life expecting miracles; this is one of them.
I was a private person before this disease. Now, in addition to the Facebook page and twitter accounts, I make use of an Instagram account (SlowItDownCKD) where I post an eye catching picture daily with the hash tag #SlowItDownCKD. This brings people to my weekly blog about CKD – as does my Instagram account as Gail Rae-Garwood – and the four books I wrote about it: one explaining it and the others the blogs in print – rather than electronic form for those who don’t have a computer or are not computer savvy. Time consuming? Oh yes, but if I expect to live a life of miracles, I need to contribute that time to share what I can about the disease and urge others to do the same.
I am urging you to realize you are the others I am asking to help cause a miracle in Chronic Kidney Disease. As the Rabbinic sage Hillel the Elder said, “If I am not for myself, who will be for me? If I am only for myself, what am I? If not now, when?” Now. You. Me. Others. CKD.
Welcome to the last blog of 2016. I find it hard to believe another year has passed, although I do acknowledge that I’m a bit slower and more content to stay in my office to write rather than run around town. It’s a bit harder to maintain my body, although my mind is doing fine… as long as I don’t have to remember too much at once, that is. Well, my knees may have something to say, but I try to keep them happy with daily exercise and the braces.
I sincerely hope you enjoyed a joyous Christmas if you celebrate. And that you continue to enjoy Chanukah and Kwanzaa (which starts today) if you celebrate. We’ll be leaving for the Trans-Siberian Orchestra concert as soon as I finish the blog… a gift from us to us and one of the kids for Christmas. On Wednesday, we’ll have our Annual Chanukah Gathering. Our New York daughter will be with us since her Chanukah gift is a plane ticket. Being a two religion family, we celebrate both Chanukah and Christmas.
Before I get to more about creating a miracle, I am proud to announce that Healthline, a trusted health information site, has named SlowItDownCKD one of The Best Kidney Disease Blogs of 2016. Talk about being surprised… and honored. Sort of a nice Christmas present, don’t you think? I suppose I can consider the publication of my novel, Portal in Time, my Chanukah present. I didn’t do too shabbily this year.
You know, it’s never too late to give either the novel or one of my Chronic Kidney Disease books as a present. Don’t forget you deserve presents, too.
Okay, on to more about miracles – or Part 2 – as I promised last week.
If CKD were common knowledge, if those in high risk categories were aware of it, we might have a chance of preventing the disease in those who don’t have it yet and/or slowing down the progression of the decline in kidney function of those who have been already diagnosed.
Exactly how can we do that? On the most basic level, there’s the spoken word. It’s not just the medical community that can talk about the disease. I can as a patient. You can, too, because you know me and I’ve told you about the disease (and/or you suffer from CKD yourself). This is most effective in areas of the world that do not have access to – or money for – doctors and treatment. This is where we can prevent more and more of the disease by preventing more and more hypertension and diabetes.
If I tell you what I know about curtailing sodium intake in high blood pressure and you tell me what you know about smoking as it contributes to hypertension, we’ve just shared two important aspects in the prevention of high blood pressure. If I tell you what I know about sugar in diabetes and you tell me what you know about carbohydrates and diabetes, we’ve just shared two important aspects in the prevention of diabetes. Then my husband starts sharing what he knows… and your third cousin once removed shares with her East Indian neighbor what her nephrologist told her… and your boss’s secretary shares what his boyfriend learned at his CKD awareness meeting, you’ve got a lot more people aware of what needs to be done about CKD. Sometimes causing a miracle is played out by sharing with people. Think of the miracle this kind of communication on a daily basis can cause.
The people you speak to will share with those they know, those they know will share with others they know until many, many more people become aware of CKD – just as that long ago Clairol hair coloring ad demonstrated how telling someone who tells someone can go on ad infinitum. Simplistic? Yes, but it works…and that’s part of living the life of causing a miracle in CKD.
Then there’s the printed word. If people are aware of CKD books and newspapers, business and educational publications can alert their populations that the disease exists and is lethal, but may be prevented and/or slowed down. Most businesses have wellness components. What perfect vehicles to transform the world’s awareness of CKD.
For example: my four Chronic Kidney Disease books are sold in 106 countries. I have 107,000 readers. This in itself is a miracle, not just for me but for everyone who is in some way connected to the disease. It is not uncommon for one community member to buy the book, then share it with everyone else in their social circle. If there’s a library, the books can be ordered and then shared for free.
These are some of the pieces I’ve written: American Kidney Fund “Slowing Down CKD – It Can Be Done” 7/14/16, Dear Annie 10/14, KidneySteps 9/11/13 & 7/4/12, National Kidney Foundation 6/6/13, It Is What It Is 3/9/12, Kevinmd.com 1/1/12, Working with Chronic Illness 1/11/10, KidneyTimes 1/11/10. Bragging? No, just demonstrating it can be done… but I had to cause it to happen by knocking on doors.
I also share my information via this blog. A doctor in a remote village in India prints and translates it to share with whichever patient has the bus fare to make it to the clinic. That patient brings the translation back to his family, friends, neighbors, and whoever else he thinks may be interested. This nephrologist’s view is the same as mine: We both need to live a life causing a miracle in Chronic Kidney Disease Awareness by sharing information. People who may not have known Chronic Kidney Disease exists now know via this sharing. Others who have undergone the simple blood and urine tests to diagnose the illness can share that the tests are not painful, other than the initial pinch of the needle for the blood draw. You would be surprised how many people, even in the high risk groups, don’t take the tests because they fear there will be pain involved. No sharing, no awareness. No awareness, no diagnose. No diagnose, no slowing down the disease.
Here are some of the blog and book mentions that have helped in my sharing of the information: Federal Register 9/25/13, The Neuropathy Doctor’s News 9/23/13, The NephCure Foundation 8/21/11, World’s Leading Expert.com 9/11/12, Glendale Community College Gaucho Gazette 8/22/11. These came about without my intervention. So what you share gets shared by others….
I’ve got some more thoughts, but we’ll have to leave them for Part 3 in the New Year. This blog is getting too long and my family is waiting for me. Happy New Year to each and every one of you. Please be safe if you’re going out to celebrate.


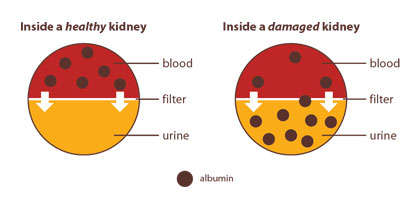
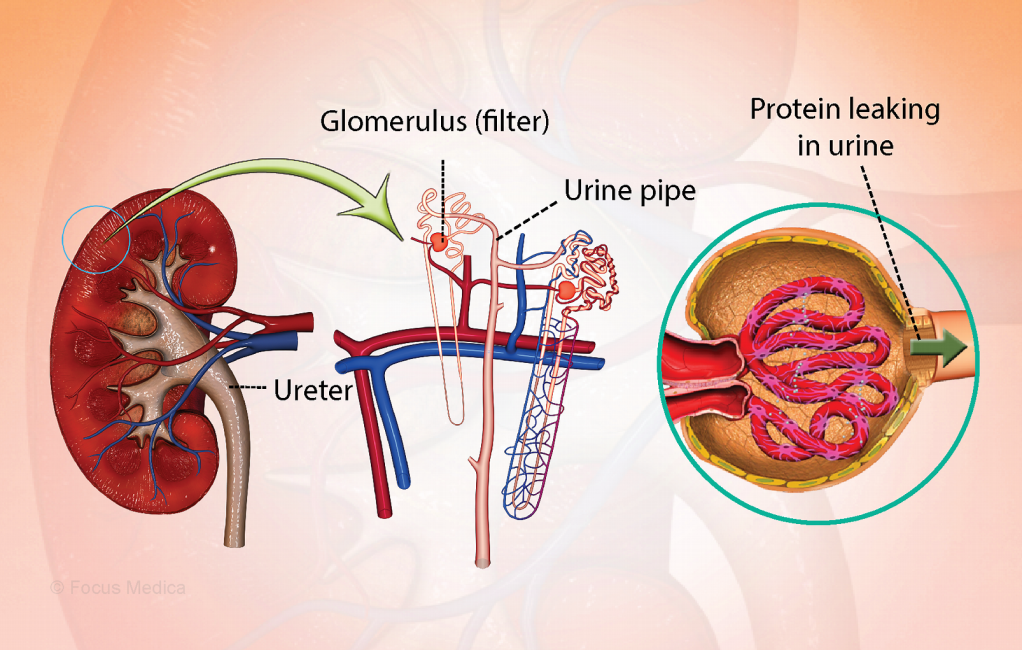
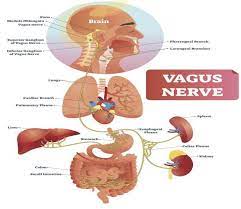
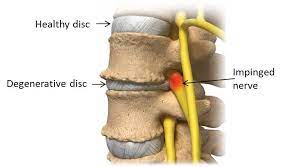

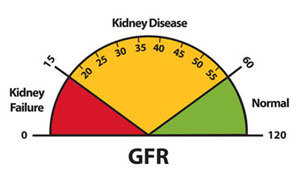
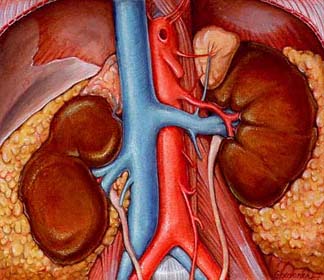








































 “Constipation can be caused by a variety of medications. These medications affect the nerve and muscle activity in the large intestine (colon) and may also bind intestinal liquid. This may result in slowed colonic action (slow and/or difficult passing of stool).”
“Constipation can be caused by a variety of medications. These medications affect the nerve and muscle activity in the large intestine (colon) and may also bind intestinal liquid. This may result in slowed colonic action (slow and/or difficult passing of stool).” 

 No, that’s not the result of misplacing my fingers on the keyboard. According to
No, that’s not the result of misplacing my fingers on the keyboard. According to 


 “Your immune system is a complex network of cells, tissues, and organs that work together to defend against germs. It helps your body to recognize these ‘foreign’ invaders. Then its job is to keep them out, or if it can’t, to find and destroy them.”
“Your immune system is a complex network of cells, tissues, and organs that work together to defend against germs. It helps your body to recognize these ‘foreign’ invaders. Then its job is to keep them out, or if it can’t, to find and destroy them.”



 “adjective
“adjective

 Do Not Smoke
Do Not Smoke

 given my work and experience on this topic.
given my work and experience on this topic.
 We all know diabetes raises your risk of developing Chronic Kidney Disease. But why? What’s the mechanism behind the fact? As far as I’m concerned, it’s time to find out.
We all know diabetes raises your risk of developing Chronic Kidney Disease. But why? What’s the mechanism behind the fact? As far as I’m concerned, it’s time to find out.

 “Dapagliflozin is used along with diet and exercise, and sometimes with other medications, to lower blood sugar levels in patients with type 2 diabetes (condition in which blood sugar is too high because the body does not produce or use insulin normally). Dapagliflozin is in a class of medications called sodium-glucose co-transporter 2 (SGLT2) inhibitors. It lowers blood sugar by causing the kidneys to get rid of more glucose in the urine. Dapagliflozin is not used to treat type 1 diabetes (condition in which the body does not produce insulin and, therefore, cannot control the amount of sugar in the blood) or diabetic ketoacidosis (a serious condition that may develop if high blood sugar is not treated).
“Dapagliflozin is used along with diet and exercise, and sometimes with other medications, to lower blood sugar levels in patients with type 2 diabetes (condition in which blood sugar is too high because the body does not produce or use insulin normally). Dapagliflozin is in a class of medications called sodium-glucose co-transporter 2 (SGLT2) inhibitors. It lowers blood sugar by causing the kidneys to get rid of more glucose in the urine. Dapagliflozin is not used to treat type 1 diabetes (condition in which the body does not produce insulin and, therefore, cannot control the amount of sugar in the blood) or diabetic ketoacidosis (a serious condition that may develop if high blood sugar is not treated).


 Let’s go to my favorite dictionary, the Merriam-Webster Dictionary at
Let’s go to my favorite dictionary, the Merriam-Webster Dictionary at 


 HERE’S THE STORY
HERE’S THE STORY
 What does CKD research typically focus on?
What does CKD research typically focus on? 
 As most of you know, I am extremely protective of my kidneys. When I was first diagnosed with Chronic Kidney Disease 11 years ago, my eGFR was only 39. Here’s a quick reminder of what the eGFR is from my first CKD book,
As most of you know, I am extremely protective of my kidneys. When I was first diagnosed with Chronic Kidney Disease 11 years ago, my eGFR was only 39. Here’s a quick reminder of what the eGFR is from my first CKD book, 
 National Kidney Month is just flying by. This is actually the last week and I doubt I’ll be able to post the rest of the 1in9 chapter before next month. But then again, it’s always Kidney Month for those of us with Chronic Kidney Disease. By the way, thank you to the reader who made it a point of telling me she can’t wait to read the rest of the chapter. Sooooo, let’s get started!
National Kidney Month is just flying by. This is actually the last week and I doubt I’ll be able to post the rest of the 1in9 chapter before next month. But then again, it’s always Kidney Month for those of us with Chronic Kidney Disease. By the way, thank you to the reader who made it a point of telling me she can’t wait to read the rest of the chapter. Sooooo, let’s get started!
 Exercise, something I loved until my arthritis got in the way, was also important. I was a dancer. Wasn’t that enough? Uh-uh, I had to learn about cardio and strength training exercise, too. It was no longer acceptable to be pleasantly plumb. My kidneys didn’t need the extra work. Hello to weights, walking, and a stationary bike. I think I took sleep for granted before CKD, too, and I now make it a point to get a good night’s sleep. A sleep apnea device improved my sleep—and my kidney function rose.
Exercise, something I loved until my arthritis got in the way, was also important. I was a dancer. Wasn’t that enough? Uh-uh, I had to learn about cardio and strength training exercise, too. It was no longer acceptable to be pleasantly plumb. My kidneys didn’t need the extra work. Hello to weights, walking, and a stationary bike. I think I took sleep for granted before CKD, too, and I now make it a point to get a good night’s sleep. A sleep apnea device improved my sleep—and my kidney function rose.
 Tomorrow is Christmas and a Merry Christmas to those of you who celebrate. The day after Christmas Kwanzaa begins, so a Happy Kwanzaa to those of you who celebrate. But back to Christmas right now: today’s blog is a present to a reader who joined me way back when I first started blogging and has since become a close online friend.
Tomorrow is Christmas and a Merry Christmas to those of you who celebrate. The day after Christmas Kwanzaa begins, so a Happy Kwanzaa to those of you who celebrate. But back to Christmas right now: today’s blog is a present to a reader who joined me way back when I first started blogging and has since become a close online friend.
 “Kidney diseases or disorders can lead to high creatinine levels. Since the kidneys are the filters of wastes from the bloodstream, kidney damage means that there will be a buildup of creatinine beside other waste products in the body. Kidney conditions such as glomerulonephritis, acute tubular necrosis, kidney infection (pyelonephritis) and kidney failure can cause high creatinine levels. Reduced blood flow to the kidneys can also have a similar effect.
“Kidney diseases or disorders can lead to high creatinine levels. Since the kidneys are the filters of wastes from the bloodstream, kidney damage means that there will be a buildup of creatinine beside other waste products in the body. Kidney conditions such as glomerulonephritis, acute tubular necrosis, kidney infection (pyelonephritis) and kidney failure can cause high creatinine levels. Reduced blood flow to the kidneys can also have a similar effect. “As the blood filtering units of your body, your kidneys are prone to problems with blood circulation and blood vessels. High blood pressure and high blood sugar can place an additional strain or burden on your kidneys. People with high blood pressure and diabetes are at a higher risk for kidney disease. People with kidney disease are at higher risk for heart and blood vessel disease. If you already have heart and blood vessel disease and kidney disease, then the body’s reactions to stress can become more and more dangerous. Therefore, whether your goal is to prevent heart and/or kidney disease, or improve your health while living with heart and/or kidney disease, managing stress is an important part of maintaining your overall health.”
“As the blood filtering units of your body, your kidneys are prone to problems with blood circulation and blood vessels. High blood pressure and high blood sugar can place an additional strain or burden on your kidneys. People with high blood pressure and diabetes are at a higher risk for kidney disease. People with kidney disease are at higher risk for heart and blood vessel disease. If you already have heart and blood vessel disease and kidney disease, then the body’s reactions to stress can become more and more dangerous. Therefore, whether your goal is to prevent heart and/or kidney disease, or improve your health while living with heart and/or kidney disease, managing stress is an important part of maintaining your overall health.” the symptoms. These are the same whether you’re the patient or the caretaker. I happen to be both a CKD patient and my Alzheimer’s husband’s caretaker, although we call me his care partner as suggested by the Alzheimer’s Association.
the symptoms. These are the same whether you’re the patient or the caretaker. I happen to be both a CKD patient and my Alzheimer’s husband’s caretaker, although we call me his care partner as suggested by the Alzheimer’s Association. Today is the last day of the eight day Chanukah celebration for us and all of you who celebrate this holiday. We usually throw a blowout party for anywhere from 30 to 50 people. But just a couple of months ago, we hosted a blowout pre-wedding potluck party for my daughter and her fiancé … and it was wonderful. Yet, it was clear that we can no longer handle undertaking such large parties. I had expressed my doubts last year about how long we’d be able to keep up the Chanukah party.
Today is the last day of the eight day Chanukah celebration for us and all of you who celebrate this holiday. We usually throw a blowout party for anywhere from 30 to 50 people. But just a couple of months ago, we hosted a blowout pre-wedding potluck party for my daughter and her fiancé … and it was wonderful. Yet, it was clear that we can no longer handle undertaking such large parties. I had expressed my doubts last year about how long we’d be able to keep up the Chanukah party.
 okay, I guess that sort of makes sense. And then, oh my, I developed diabetes. But how? I’d never questioned how that worked before, but I certainly did now.
okay, I guess that sort of makes sense. And then, oh my, I developed diabetes. But how? I’d never questioned how that worked before, but I certainly did now. Guilty on all three counts as far as symptoms. It gets worse. I uncovered this fact in
Guilty on all three counts as far as symptoms. It gets worse. I uncovered this fact in 
 I would say I’m heart… uh, kidney…broken about this development, but the truth is I’m not. I don’t like it; I don’t want it, but I can do something about it. I’d already cut out complex carbs and sugar laden foods in an abortive attempt to lose weight for my health. Well, maybe my daughter’s wedding on October 6th had something to do with that decision, too.
I would say I’m heart… uh, kidney…broken about this development, but the truth is I’m not. I don’t like it; I don’t want it, but I can do something about it. I’d already cut out complex carbs and sugar laden foods in an abortive attempt to lose weight for my health. Well, maybe my daughter’s wedding on October 6th had something to do with that decision, too.


 suggesting I do so for years, but I’m not a joiner. Let’s change that; I wasn’t a joiner. The AAKP conference made the difference.
suggesting I do so for years, but I’m not a joiner. Let’s change that; I wasn’t a joiner. The AAKP conference made the difference.


 When I was a little girl, I liked to listen to my father whistle ‘All of Me,’ written by Marks and Simon in 1931 when Charlie, my father, was just 16. Only a few years later, it became a sort of love language for my mother and him. Enter a former husband of my own and my children. When my folks visited from Florida and my then husband’s side of the family journeyed over to Staten Island from Brooklyn to visit them, they all sang the song with great emotion. (By then, Bell’s palsy had robbed my father of the ability to whistle.)
When I was a little girl, I liked to listen to my father whistle ‘All of Me,’ written by Marks and Simon in 1931 when Charlie, my father, was just 16. Only a few years later, it became a sort of love language for my mother and him. Enter a former husband of my own and my children. When my folks visited from Florida and my then husband’s side of the family journeyed over to Staten Island from Brooklyn to visit them, they all sang the song with great emotion. (By then, Bell’s palsy had robbed my father of the ability to whistle.)
 Better Information
Better Information
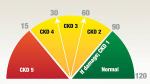 decline in our kidney function. I maintain that if only my primary care physician had told me when he first noticed that 39% GFR, maybe I wouldn’t be in stage 3 of 5. Maybe those now on dialysis or searching for a transplant wouldn’t be in the position they are, either.
decline in our kidney function. I maintain that if only my primary care physician had told me when he first noticed that 39% GFR, maybe I wouldn’t be in stage 3 of 5. Maybe those now on dialysis or searching for a transplant wouldn’t be in the position they are, either.
 The literature suggests early nephrologist involvement improves long-term outcomes. Proactive primary care offers longitudinal guidance for making the enormous lifestyle changes in diet, exercise, stress management, hydration, sleep and toxic exposures, while offering psychological counseling that is required to achieve such changes. The cross-over benefits for patients’ other diagnoses is well known.
The literature suggests early nephrologist involvement improves long-term outcomes. Proactive primary care offers longitudinal guidance for making the enormous lifestyle changes in diet, exercise, stress management, hydration, sleep and toxic exposures, while offering psychological counseling that is required to achieve such changes. The cross-over benefits for patients’ other diagnoses is well known. surgeries, travel and stress — need to grasp a breadth of nephrology basics. Our patients with CKD are at increased risk of acute kidney injury. Astute protection means we save nephrons. This author would welcome renal rotations at all levels of medical training, with a facet of focus on longitudinal outpatient, early and moderate CKD care. This vision of collaboration, with a commitment to early diagnosis and intervention, offers the opportunity to learn how to guide patients to a less inflammatory lifestyle.
surgeries, travel and stress — need to grasp a breadth of nephrology basics. Our patients with CKD are at increased risk of acute kidney injury. Astute protection means we save nephrons. This author would welcome renal rotations at all levels of medical training, with a facet of focus on longitudinal outpatient, early and moderate CKD care. This vision of collaboration, with a commitment to early diagnosis and intervention, offers the opportunity to learn how to guide patients to a less inflammatory lifestyle.




 This is from
This is from 
 It looks like I was wrong. Most of these are still available. Unfortunately KidneyDiet, my all-time favorite, is no more. Neither is Restaurant Nutrition. But let’s see what other apps are available for us.
It looks like I was wrong. Most of these are still available. Unfortunately KidneyDiet, my all-time favorite, is no more. Neither is Restaurant Nutrition. But let’s see what other apps are available for us. request reminders about your goal, as well as add foods. Of course, Premium offers you a lot more… and charges you accordingly. Articles about exercise and weight pop up, too. And then there are recipes. Again, it doesn’t do the whole trick, although it does count potassium, protein, sodium and calories . What’s missing is phosphorous. The bonuses are carb, fat (by type, no less) cholesterol, fiber, sugar, vitamins A & C, calcium, and iron counters. This is also a free Apple app.
request reminders about your goal, as well as add foods. Of course, Premium offers you a lot more… and charges you accordingly. Articles about exercise and weight pop up, too. And then there are recipes. Again, it doesn’t do the whole trick, although it does count potassium, protein, sodium and calories . What’s missing is phosphorous. The bonuses are carb, fat (by type, no less) cholesterol, fiber, sugar, vitamins A & C, calcium, and iron counters. This is also a free Apple app. Before I go, here’s a shameless plug for my new book. It’s
Before I go, here’s a shameless plug for my new book. It’s  I was going to give you my take on researching when I stumbled across Dr. Alicia White’s piece on the United Kingdom’s National Health Services site at
I was going to give you my take on researching when I stumbled across Dr. Alicia White’s piece on the United Kingdom’s National Health Services site at 
 Also, it’s important that the control group is as similar to the treated/exposed group as possible. The best way to achieve this is to randomly assign some people to be in the treated/exposed group and some people to be in the control group. This is what happens in a randomised controlled trial (RCT) and is why RCTs are considered the “gold standard” for testing the effects of treatments and exposures. … Without either, retain some healthy scepticism.
Also, it’s important that the control group is as similar to the treated/exposed group as possible. The best way to achieve this is to randomly assign some people to be in the treated/exposed group and some people to be in the control group. This is what happens in a randomised controlled trial (RCT) and is why RCTs are considered the “gold standard” for testing the effects of treatments and exposures. … Without either, retain some healthy scepticism.
 What is an endoscopy, you ask. According to the Mayo Clinic at
What is an endoscopy, you ask. According to the Mayo Clinic at 




 According to the Kidney Foundation of Canada at
According to the Kidney Foundation of Canada at 

 Learning to read a Nutrition Facts label is a must if the doctor wants to do all he or she can to help the patient slow down – and sometimes halt – the progression of kidney disease. It is important to remember that in the earlier stages of kidney disease, the diet may not be as strict – but if progression of the disease is noted, then dietary modifications are more stringent and frequent laboratory tests may need to be performed to assess progress.
Learning to read a Nutrition Facts label is a must if the doctor wants to do all he or she can to help the patient slow down – and sometimes halt – the progression of kidney disease. It is important to remember that in the earlier stages of kidney disease, the diet may not be as strict – but if progression of the disease is noted, then dietary modifications are more stringent and frequent laboratory tests may need to be performed to assess progress. over the counter medications that may harm your kidneys such as Advil, Motrin, Aleve, Ibuprofen, Celebrex, Prilosec, herbal remedies, etc. I encourage all patients to memorize their medications and keep a list with them at all times. Remember that all medications are prescribed because the benefit to the patient outweighs the risk and no medication is entirely safe; therefore, it should be taken as prescribed and any side effects reported to your doctor. You should not take any new medicine unless it has been cleared by your kidney specialist.
over the counter medications that may harm your kidneys such as Advil, Motrin, Aleve, Ibuprofen, Celebrex, Prilosec, herbal remedies, etc. I encourage all patients to memorize their medications and keep a list with them at all times. Remember that all medications are prescribed because the benefit to the patient outweighs the risk and no medication is entirely safe; therefore, it should be taken as prescribed and any side effects reported to your doctor. You should not take any new medicine unless it has been cleared by your kidney specialist.
































{kind=link}